
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager

Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Childhood obesity: A review of current and future management options
Affiliations.
- 1 Department of Paediatric Endocrinology, Alder Hey Children's Hospital, Liverpool, UK.
- 2 Centre for Endocrinology, William Harvey Research Institute, Barts and the London School of Medicine, Queen Mary University of London, London, UK.
- 3 Department of Paediatric Dietetics, Alder Hey Children's Hospital, Liverpool, UK.
- 4 Department of Paediatric Clinical Psychology, Alder Hey Children's Hospital, Liverpool, UK.
- PMID: 34750858
- DOI: 10.1111/cen.14625
Obesity is becoming increasingly prevalent in paediatric populations worldwide. In addition to increasing prevalence, the severity of obesity is also continuing to rise. Taken together, these findings demonstrate a worrying trend and highlight one of the most significant challenges to public health. Childhood obesity affects multiple organs in the body and is associated with both significant morbidity and ultimately premature mortality. The prevalence of complications associated with obesity, including dyslipidaemia, hypertension, fatty liver disease and psychosocial complications are becoming increasingly prevalent within the paediatric populations. Treatment guidelines currently focus on intervention with lifestyle and behavioural modifications, with pharmacotherapy and surgery reserved for patients who are refractory to such treatment. Research into adult obesity has established pharmacological novel therapies, which have been approved and established in clinical practice; however, the research and implementation of such therapies in paediatric populations have been lagging behind. Despite the relative lack of widespread research in comparison to the adult population, newer therapies are being trialled, which should allow a greater availability of treatment options for childhood obesity in the future. This review summarizes the current evidence for the management of obesity in terms of medical and surgical options. Both future therapeutic agents and those which cause weight loss but have an alternative indication are also included and discussed as part of the review. The review summarizes the most recent research for each intervention and demonstrates the potential efficacy and limitations of each treatment option.
Keywords: BMI; childhood obesity; lifestyle interventions; paediatrics; pharmacotherapy.
© 2021 John Wiley & Sons Ltd.
PubMed Disclaimer
Similar articles
- The effectiveness of web-based programs on the reduction of childhood obesity in school-aged children: A systematic review. Antwi F, Fazylova N, Garcon MC, Lopez L, Rubiano R, Slyer JT. Antwi F, et al. JBI Libr Syst Rev. 2012;10(42 Suppl):1-14. doi: 10.11124/jbisrir-2012-248. JBI Libr Syst Rev. 2012. PMID: 27820152
- Treatment Options for Severe Obesity in the Pediatric Population: Current Limitations and Future Opportunities. Ryder JR, Fox CK, Kelly AS. Ryder JR, et al. Obesity (Silver Spring). 2018 Jun;26(6):951-960. doi: 10.1002/oby.22196. Epub 2018 May 7. Obesity (Silver Spring). 2018. PMID: 29732716 Review.
- The future of Cochrane Neonatal. Soll RF, Ovelman C, McGuire W. Soll RF, et al. Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
- Real-World Strategies to Treat Hypertension Associated with Pediatric Obesity. Binka E, Brady TM. Binka E, et al. Curr Hypertens Rep. 2019 Feb 12;21(2):18. doi: 10.1007/s11906-019-0922-2. Curr Hypertens Rep. 2019. PMID: 30747290 Free PMC article. Review.
- Screening and Interventions for Childhood Overweight [Internet]. Whitlock EP, Williams SB, Gold R, Smith P, Shipman S. Whitlock EP, et al. Rockville (MD): Agency for Healthcare Research and Quality (US); 2005 Jul. Rockville (MD): Agency for Healthcare Research and Quality (US); 2005 Jul. PMID: 20722132 Free Books & Documents. Review.
- Is oxidative stress - antioxidants imbalance the physiopathogenic core in pediatric obesity? Lupu A, Fotea S, Jechel E, Starcea IM, Ioniuc I, Knieling A, Salaru DL, Sasaran MO, Cirstea O, Revenco N, Mihai CM, Lupu VV, Nedelcu AH. Lupu A, et al. Front Immunol. 2024 Aug 8;15:1394869. doi: 10.3389/fimmu.2024.1394869. eCollection 2024. Front Immunol. 2024. PMID: 39176098 Free PMC article. Review.
- The Prevention of Childhood Obesity Is a Priority: The Preliminary Results of the "EpPOI: Education to Prevent Childhood Obesity" Project. Porri D, Luppino G, Morabito LA, La Rosa E, Pepe G, Corica D, Valenzise M, Messina MF, Zirilli G, Li Pomi A, Alibrandi A, Di Mauro D, Aversa T, Wasniewska MG. Porri D, et al. Nutrients. 2024 Aug 2;16(15):2538. doi: 10.3390/nu16152538. Nutrients. 2024. PMID: 39125417 Free PMC article.
- Comparative Efficacy and Safety of Glucagon-like Peptide-1 Receptor Agonists in Children and Adolescents with Obesity or Overweight: A Systematic Review and Network Meta-Analysis. Liu L, Shi H, Shi Y, Wang A, Guo N, Tao H, Nahata MC. Liu L, et al. Pharmaceuticals (Basel). 2024 Jun 24;17(7):828. doi: 10.3390/ph17070828. Pharmaceuticals (Basel). 2024. PMID: 39065679 Free PMC article. Review.
- Analysis of Prescription Trends for Narcotic Appetite Suppressants: Utilizing the Narcotics Information Management System. Oh KS, Han E. Oh KS, et al. Yonsei Med J. 2024 Aug;65(8):480-487. doi: 10.3349/ymj.2023.0335. Yonsei Med J. 2024. PMID: 39048324 Free PMC article.
- The Impact of Excessive Fructose Intake on Adipose Tissue and the Development of Childhood Obesity. Azevedo-Martins AK, Santos MP, Abayomi J, Ferreira NJR, Evangelista FS. Azevedo-Martins AK, et al. Nutrients. 2024 Mar 25;16(7):939. doi: 10.3390/nu16070939. Nutrients. 2024. PMID: 38612973 Free PMC article. Review.
- NHS Digital. National Statistics: National Child Measurement Programme, England. 2017/18. Accessed April, 2021. https://digital.nhs.uk/data-and-information/publications/statistical/nat...
- Viner RM, Kinra S, Christie D, et al. Improving the assessment and management of obesity in UK children and adolescents: the PROMISE research programme including a RCT. Programme Grants for Applied Research, No. 8.3. 2020.
- Baker C. Briefing paper: obesity statistics. House of Commons Library. 2019;3336:1-20.
- Styne DM, Arslanian SA, Connor EL, et al. Pediatric obesity-assessment, treatment, and prevention: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2017;102(3):709-757.
- Gungor NK. Overweight and obesity in children and adolescents. J Clin Res Pediatr Endocrinol. 2014;6(3):129-143.
Publication types
- Search in MeSH
Related information
Linkout - more resources, full text sources.
- Ovid Technologies, Inc.
- MedlinePlus Health Information

- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
- Funding Opportunities
Accelerating Progress to Reduce Childhood Obesity
Explore the many products nccor has created over the past decade.
Want To Know More?
Stay up to date

FEATURED TOOL
Catalogue of Surveillance Systems
Increase efficiency with access over 100 surveillance systems relevant to childhood obesity research— now featuring variables for sleep research!
Additional tools

Research articles

Featured Publication
2023 annual report, news & webinars.
E-Newsletter
September 2024
NCCOR E-newsletter
August 2024
New nccor research presented at isbnpa 2024.
May 22, 2024
Obesity-Related Policy, Systems, and Environmental Research in the U.S. (OPUS)
June 4-5, 2024
Register Today! Upcoming NCCOR Workshop Examines Obesity Prevention Research, Community Engagement, and Systems Change
May 06, 2024
Celebrating a Milestone: NCCOR’s 2023 Annual Report Showcases Strategic Impact on Childhood Obesity Research
Apr 12, 2024
Sleep’s Role in Child Health: Expanding NCCOR’s Catalogue of Surveillance Systems
March 13, 2024 -
Never miss a newsletter
We are social.
Check us out on Facebook, LinkedIn, Twitter and YouTube
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Published: 18 May 2023
Child and adolescent obesity
- Natalie B. Lister ORCID: orcid.org/0000-0002-9148-8632 1 , 2 ,
- Louise A. Baur ORCID: orcid.org/0000-0002-4521-9482 1 , 3 , 4 ,
- Janine F. Felix 5 , 6 ,
- Andrew J. Hill ORCID: orcid.org/0000-0003-3192-0427 7 ,
- Claude Marcus ORCID: orcid.org/0000-0003-0890-2650 8 ,
- Thomas Reinehr ORCID: orcid.org/0000-0002-4351-1834 9 ,
- Carolyn Summerbell 10 &
- Martin Wabitsch ORCID: orcid.org/0000-0001-6795-8430 11
Nature Reviews Disease Primers volume 9 , Article number: 24 ( 2023 ) Cite this article
48k Accesses
95 Citations
251 Altmetric
Metrics details
- Paediatric research
The prevalence of child and adolescent obesity has plateaued at high levels in most high-income countries and is increasing in many low-income and middle-income countries. Obesity arises when a mix of genetic and epigenetic factors, behavioural risk patterns and broader environmental and sociocultural influences affect the two body weight regulation systems: energy homeostasis, including leptin and gastrointestinal tract signals, operating predominantly at an unconscious level, and cognitive–emotional control that is regulated by higher brain centres, operating at a conscious level. Health-related quality of life is reduced in those with obesity. Comorbidities of obesity, including type 2 diabetes mellitus, fatty liver disease and depression, are more likely in adolescents and in those with severe obesity. Treatment incorporates a respectful, stigma-free and family-based approach involving multiple components, and addresses dietary, physical activity, sedentary and sleep behaviours. In adolescents in particular, adjunctive therapies can be valuable, such as more intensive dietary therapies, pharmacotherapy and bariatric surgery. Prevention of obesity requires a whole-system approach and joined-up policy initiatives across government departments. Development and implementation of interventions to prevent paediatric obesity in children should focus on interventions that are feasible, effective and likely to reduce gaps in health inequalities.
Similar content being viewed by others

Management for children and adolescents with overweight and obesity: a recommendations mapping

Unraveling Complexity about Childhood Obesity and Nutritional Interventions: Modeling Interactions Among Psychological Factors

Pediatric weight management interventions improve prevalence of overeating behaviors
Introduction.
The prevalence of child and adolescent obesity remains high and continues to rise in low-income and middle-income countries (LMICs) at a time when these regions are also contending with under-nutrition in its various forms 1 , 2 . In addition, during the COVID-19 pandemic, children and adolescents with obesity have been more likely to have severe COVID-19 requiring hospitalization and mechanical ventilation 3 . At the same time, the pandemic was associated with rising levels of childhood obesity in many countries. These developments are concerning, considering that recognition is also growing that paediatric obesity is associated with a range of immediate and long-term negative health outcomes, a decreased quality of life 4 , 5 , an increased presentation to health services 6 and increased economic costs to individuals and society 7 .
Body weight is regulated by a range of energy homeostatic and cognitive–emotional processes and a multifactorial interplay of complex regulatory circuits 8 . Paediatric obesity arises when multiple environmental factors — covering preconception and prenatal exposures, as well as broader changes in the food and physical activity environments — disturb these regulatory processes; these influences are now widespread in most countries 9 .
The treatment of obesity includes management of obesity-associated complications, a developmentally sensitive approach, family engagement, and support for long-term behaviour changes in diet, physical activity, sedentary behaviours and sleep 10 . New evidence highlights the role, in adolescents with more severe obesity, of bariatric surgery 11 and pharmacotherapy, particularly the potential for glucagon-like peptide 1 (GLP1) receptor agonists 12 .
Obesity prevention requires a whole-system approach, with policies across all government and community sectors systematically taking health into account, avoiding harmful health impacts and decreasing inequity. Programmatic prevention interventions operating ‘downstream’ at the level of the child and family, as well as ‘upstream’ interventions at the level of the community and broader society, are required if a step change in tackling childhood obesity is to be realized 13 , 14 .
In this Primer, we provide an overview of the epidemiology, causes, pathophysiology and consequences of child and adolescent obesity. We discuss diagnostic considerations, as well as approaches to its prevention and management. Furthermore, we summarize effects of paediatric obesity on quality of life, and open research questions.
Epidemiology
Definition and prevalence.
The World Health Organization (WHO) defines obesity as “abnormal or excessive fat accumulation that presents a risk to health” 15 . Paediatric obesity is defined epidemiologically using BMI, which is adjusted for age and sex because of the physiological changes in BMI during growth 16 . Global prevalence of paediatric obesity has risen markedly over the past four decades, initially in high-income countries (HICs), but now also in many LMICs 1 .
Despite attempts to standardize the epidemiological classification, several definitions of paediatric obesity are in use; hence, care is needed when comparing prevalence rates. The 2006 WHO Child Growth Standard, for children aged 0 to 5 years, is based on longitudinal observations of multiethnic populations of children with optimal infant feeding and child-rearing conditions 17 . The 2007 WHO Growth Reference is used for the age group 5–19 years 18 , and the 2000 US Centers for Disease Control and Prevention (CDC) Growth Charts for the age group 2–20 years 19 . The WHO and CDC definitions based on BMI-for-age charts are widely used, including in clinical practice. By contrast, the International Obesity Task Force (IOTF) definition, developed from nationally representative BMI data for the age group 2–18 years from six countries, is used exclusively for epidemiological studies 20 .
For the age group 5–19 years, between 1975 and 2016, the global prevalence of obesity (BMI >2 standard deviations (SD) above the median of the WHO growth reference) increased around eightfold to 5.6% in girls and 7.8% in boys 1 . Rates have plateaued at high levels in many HICs but have accelerated in other regions, particularly in parts of Asia. For the age group 2–4 years, between 1980 and 2015, obesity prevalence (IOTF definition, equivalent to an adult BMI of ≥30 kg/m 2 ) increased from 3.9% to 7.2% in boys and from 3.7% to 6.4% in girls 21 . Obesity prevalence is highest in Polynesia and Micronesia, the Middle East and North Africa, the Caribbean and the USA (Fig. 1 ). Variations in prevalence probably reflect different background levels of obesogenic environments, or the sum total of the physical, economic, policy, social and cultural factors that promote obesity 22 . Obesogenic environments include those with decreased active transport options, a ubiquity of food marketing directed towards children, and reduced costs and increased availability of nutrient-poor, energy-dense foods. Particularly in LMICs, the growth of urbanization, new forms of technology and global trade have led to reduced physical activity at work and leisure, a shift towards Western diets, and the expansion of transnational food and beverage companies to shape local food systems 23 .

Maps showing the proportions of children and adolescents living with overweight or obesity (part a , boys; part b , girls) according to latest available data from the Global Obesity Observatory . Data might not be comparable between countries owing to differences in survey methodology.
The reasons for varying sex differences in prevalence in different countries are unclear but may relate to cultural variations in parental feeding practices for boys and girls and societal ideals of body size 24 . In 2016, obesity in the age group 5–19 years was more prevalent in girls than in boys in sub-Saharan Africa, Oceania and some middle-income countries in other regions, whereas it was more prevalent in boys than in girls in all HICs, and in East and South-East Asia 21 . Ethnic and racial differences in obesity prevalence within countries are often assumed to mirror variations in social deprivation and other social determinants of obesity. However, an independent effect of ethnicity even after adjustment for socioeconomic status has been documented in the UK, with Black and Asian boys in primary school having higher prevalence of obesity than white boys 25 .
Among individuals with obesity, very high BMI values have become more common in the past 15 years. The prevalence of severe obesity (BMI ≥120% of the 95th percentile (CDC definition), or ≥35 kg/m 2 at any age 26 , 27 ) has increased in many HICs, accounting for one-quarter to one-third of those with obesity 28 , 29 . Future health risks of paediatric obesity in adulthood are well documented. For example, in a data linkage prospective study in Israel with 2.3 million participants who had BMI measured at age 17 years, those with obesity (≥95th percentile BMI for age) had a much higher risk of death from coronary heart disease (HR 4.9, 95% CI 3.9–6.1), stroke (HR 2.6, 95% CI 1.7–4.1) and sudden death (HR 2.1, 95% CI 1.5–2.9) compared with those whose BMI fell between the 5th and 24th percentiles 30 .
Causes and risk factors
Early life is a critical period for childhood obesity development 9 , 31 , 32 , 33 . According to the Developmental Origins of Health and Disease framework, the early life environment may affect organ structure and function and influence health in later life 34 , 35 . Meta-analyses have shown that preconception and prenatal environmental exposures, including high maternal pre-pregnancy BMI and, to a lesser extent, gestational weight gain, as well as gestational diabetes and maternal smoking, are associated with childhood obesity, potentially through effects on the in utero environment 33 , 36 , 37 , 38 . Paternal obesity is also associated with childhood obesity 33 . Birthweight, reflecting fetal growth, is a proxy for in utero exposures. Both low and high birthweights are associated with later adiposity, with high birthweight linked to increased BMI and low birthweight to central obesity 33 , 39 .
Growth trajectories in early life are important determinants of later adiposity. Rapid weight gain in early childhood is associated with obesity in adolescence 32 . Also, later age and higher BMI at adiposity peak (the usual peak in BMI around 9 months of age), as well as earlier age at adiposity rebound (the lowest BMI reached between 4 and 7 years of age), are associated with increased adolescent and adult BMI 40 , 41 . Specific early life nutritional factors, including a lower protein content in formula food, are consistently associated with a lower risk of childhood obesity 42 , 43 . These also include longer breastfeeding duration, which is generally associated with a lower risk of childhood obesity 42 . However, some controversy exists, as these effects are affected by multiple sociodemographic confounding factors and their underlying mechanisms remain uncertain 44 . Some studies comparing higher and lower infant formula protein content have reported that the higher protein group have a greater risk of subsequent obesity, especially in early childhood 41 , 42 ; however, one study with a follow-up period until age 11 years found no significant difference in the risk of obesity, but an increased risk of overweight in the high protein group was still observed 42 , 43 , 45 . A high intake of sugar-sweetened beverages is associated with childhood obesity 33 , 46 .
Many other behavioural factors are associated with an increased risk of childhood obesity, including increased screen time, short sleep duration and poor sleep quality 33 , 47 , reductions in physical activity 48 and increased intake of energy-dense micronutrient-poor foods 49 . These have been influenced by multiple changes in the past few decades in the broader social, economic, political and physical environments, including the widespread marketing of food and beverages to children, the loss of walkable green spaces in many urban environments, the rise in motorized transport, rapid changes in the use of technology, and the move away from traditional foods to ultraprocessed foods.
Obesity prevalence is inextricably linked to relative social inequality, with data suggesting a shift in prevalence over time towards those living with socioeconomic disadvantage, and thus contributes to social inequalities. In HICs, being in lower social strata is associated with a higher risk of obesity, even in infants and young children 50 , whereas the opposite relationship occurs in middle-income countries 51 . In low-income countries, the relationship is variable, and the obesity burden seems to be across socioeconomic groups 52 , 53 .
Overall, many environmental, lifestyle, behavioural and social factors in early life are associated with childhood obesity. These factors cannot be seen in isolation but are part of a complex interplay of exposures that jointly contribute to increased obesity risk. In addition to multiple prenatal and postnatal environmental factors, genetic variants also have a role in the development of childhood obesity (see section Mechanisms/pathophysiology).
Comorbidities and complications
Childhood obesity is associated with a wide range of short-term comorbidities (Fig. 2 ). In addition, childhood obesity tracks into adolescence and adulthood and is associated with complications across the life course 32 , 41 , 54 , 55 .

Obesity in children and adolescents can be accompanied by various other pathologies. In addition, childhood obesity is associated with complications and disorders that manifest in adulthood (red box).
Increased BMI, especially in adolescence, is linked to a higher risk of many health outcomes, including metabolic disorders, such as raised fasting glucose, impaired glucose tolerance, type 2 diabetes mellitus (T2DM), metabolic syndrome and fatty liver disease 56 , 57 , 58 , 59 . Other well-recognized obesity-associated complications include coronary heart disease, asthma, obstructive sleep apnoea syndrome (itself associated with metabolic dysfunction and inflammation) 60 , orthopaedic complications and a range of mental health outcomes including depression and low self-esteem 27 , 55 , 57 , 61 , 62 , 63 .
A 2019 systematic review showed that children and adolescents with obesity are 1.4 times more likely to have prediabetes, 1.7 times more likely to have asthma, 4.4 times more likely to have high blood pressure and 26.1 times more likely to have fatty liver disease than those with a healthy weight 64 . In 2016, it was estimated that, at a global level by 2025, childhood obesity would lead to 12 million children aged 5–17 years with glucose intolerance, 4 million with T2DM, 27 million with hypertension and 38 million with fatty liver disease 65 . These high prevalence rates have implications for both paediatric and adult health services.
Mechanisms/pathophysiology
Body weight regulation.
Body weight is regulated within narrow limits by homeostatic and cognitive–emotional processes and a multifactorial interplay of hormones and messenger substances in complex regulatory circuits (Fig. 3 ). When these regulatory circuits are disturbed, an imbalance between energy intake and expenditure leads to obesity or to poor weight gain. As weight loss is much harder to achieve than weight gain in the long term due to the regulation circuits discussed below, the development of obesity is encouraged by modern living conditions, which enable underlying predispositions for obesity to become manifest 8 , 66 .

Body weight is predominantly regulated by two systems: energy homeostasis and cognitive–emotional control. Both homeostatic and non-homeostatic signals are processed in the brain, involving multiple hormone and receptor cascades 217 , 218 , 219 . This overview depicts the best-known regulatory pathways. The homeostatic system, which is mainly regulated by brain centres in the hypothalamus and brainstem, operates on an unconscious level. Both long-term signals from the energy store in adipose tissue (for example, leptin) and short-term hunger and satiety signals from the gastrointestinal tract signal the current nutrient status. During gastric distension or after the release of gastrointestinal hormones (multiple receptors are involved) and insulin, a temporary feeling of fullness is induced. The non-homeostatic or hedonic system is regulated by higher-level brain centres and operates at the conscious level. After integration in the thalamus, homeostatic signals are combined with stimuli from the environment, experiences and emotions; emotional and cognitive impulses are then induced to control food intake. Regulation of energy homeostasis in the hypothalamus involves two neuron types of the arcuate nucleus: neurons producing neuropeptide Y (NPY) and agouti-related peptide (AgRP) and neurons producing pro-opiomelanocortin (POMC). Leptin stimulates these neurons via specific leptin receptors (LEPR) inducing anabolic effects in case of decreasing leptin levels and catabolic effects in case of increasing leptin levels. Leptin inhibits the production of NPY and AgRP, whereas low leptin levels stimulate AgRP and NPY production resulting in the feeling of hunger. Leptin directly stimulates POMC production in POMC neurons. POMC is cleaved into different hormone polypeptides including α-melanocyte-stimulating hormone which in turn activates melanocortin 4 receptors (MC4R) of cells in the nucleus paraventricularis of the hypothalamus, leading to the feeling of satiety. CART, cocaine and amphetamine responsive transcript; IR, insulin receptor.
In principle, there are two main systems in the brain which regulate body weight 8 , 66 (Fig. 3 ): energy homeostasis and cognitive–emotional control. Energy homeostasis is predominantly regulated by brain centres in the hypothalamus and brainstem and operates at an unconscious level. Both long-term signals from the adipose tissue energy stores and short-term hunger and satiety signals from the gastrointestinal tract signal the current nutrient status 8 , 66 . For example, negative energy balance leading to reduced fat mass results in reduced leptin levels, a permanently reduced urge to exercise and an increased feeling of hunger. During gastric distension or after the release of gastrointestinal hormones and insulin, a temporary feeling of fullness is induced 8 , 66 . Cognitive–emotional control is regulated by higher brain centres and operates at a conscious level. Here, the homeostatic signals are combined with stimuli from the environment (sight, smell and taste of food), experiences and emotions 8 , 66 . Disorders at the level of cognitive–emotional control mechanisms include emotional eating as well as eating disorders. For example, the reward areas in the brain of people with overweight are more strongly activated by high-calorie foods than those in the brain of people with normal weight 67 . Both systems interact with each other, and the cognitive–emotional system is strongly influenced by the homeostatic control circuits.
Disturbances in the regulatory circuits of energy homeostasis can be genetically determined, can result from disease or injury to the regulatory centres involved, or can be caused by prenatal programming 8 , 66 . If the target value of body weight has been shifted, the organism tries by all means (hunger, drive) to reach the desired higher weight. These disturbed signals of the homeostatic system can have an imperative, irresistible character, so that a conscious influence on food intake is no longer effectively possible 8 , 66 . The most important disturbances of energy homeostasis are listed in Table 1 .
The leptin pathway
The peptide hormone leptin is primarily produced by fat cells. Its production depends on the amount of adipose tissue and the energy balance. A negative energy balance during fasting results in a reduction of circulating leptin levels by 50% after 24 h (ref. 68 ). In a state of weight loss, leptin production is reduced 69 . In the brain, leptin stimulates two neuron types of the arcuate nucleus in the hypothalamus via specific leptin receptors: neurons producing neuropeptide Y (NPY) and agouti-related peptide (AgRP) and neurons producing pro-opiomelanocortin (POMC). High leptin levels inhibit the production of NPY and AgRP, whereas low leptin levels stimulate AgRP and NPY production. By contrast, leptin directly stimulates POMC production in POMC neurons (Fig. 3 ). POMC is a hormone precursor that is cleaved into different hormone polypeptides by specific enzymes, such as prohormone convertase 1 (PCSK1). This releases α-melanocyte-stimulating hormone (α-MSH) which in turn activates melanocortin 4 receptors (MC4R) of cells in the nucleus paraventricularis of the hypothalamus, leading to the feeling of satiety. Rare, functionally relevant mutations in the genes for leptin and leptin receptor, POMC , PCSK1/3 or MC4R lead to extreme obesity in early childhood. These forms of obesity are potential indications for specific pharmacological treatments, for example setmelanotide 70 , 71 . MC4R mutations are the most common cause of monogenic obesity, as heterozygous mutations can be symptomatic depending on the functional impairment and with variable penetrance and expression. Other genes have been identified, in which rare heterozygous pathological variants are also associated with early onset obesity (Table 1 ).
Pathological changes in adipose tissue
Adipose tissue can be classified into two types, white and brown adipose tissue. White adipose tissue comprises unilocular fat cells and brown adipose tissue contains multilocular fat cells, which are rich in mitochondria 72 . A third type of adipocyte, beige adipocytes, within the white adipose tissue are induced by prolonged exposure to cold or adrenergic signalling, and show a brown adipocyte-like morphology 72 . White adipose tissue has a large potential to change its volume to store energy and meet the metabolic demands of the body. The storage capacity and metabolic function of adipose tissue depend on the anatomical location of the adipose tissue depot. Predominant enlargement of white adipose tissue in the visceral, intra-abdominal area (central obesity) is associated with insulin resistance and an increased risk of metabolic disease development before puberty. Accumulation of adipose tissue in the hips and flanks has no adverse effect and may be protective against metabolic syndrome. In those with obesity, adipose tissue is characterized by an increased number of adipocytes (hyperplasia), which originate from tissue-resident mesenchymal stem cells, and by enlarged adipocytes (hypertrophy) 73 . Adipocytes with a very large diameter reach the limit of the maximal oxygen diffusion distance, resulting in hypoxia, the development of an inflammatory expression profile (characterized by, for example, leptin, TNF and IL-6) and adipocyte necrosis, triggering the recruitment of leukocytes. Resident macrophages switch from the anti-inflammatory M2 phenotype to a pro-inflammatory M1 phenotype, which is associated with insulin resistance, further promoting local sterile inflammation and the development of fibrotic adipose tissue. This process limits the expandability of the adipose tissue for further storage of triglycerides. In the patient, the increase in fat mass in obesity is associated with insulin resistance and systemic low-grade inflammation characterized by elevated serum levels of C-reactive protein and pro-inflammatory cytokines. The limitation of adipose tissue expandability results in storage of triglycerides in other organs, such as the liver, muscle and pancreas 74 .
Genetics and epigenetics in the general population
Twin studies have found heritability estimates for BMI of up to 70% 75 , 76 . In contrast to rare monogenic forms of obesity, which are often caused by a single genetic defect with a large effect, the genetic background of childhood obesity in the general population is shaped by the joint effects of many common genetic variants, each of which individually makes a small contribution to the phenotype. For adult BMI, genome-wide association studies, which examine associations of millions of such variants across the genome at the same time, have identified around 1,000 genetic loci 77 . The largest genome-wide association studies in children, which include much smaller sample sizes of up to 60,000 children, have identified 25 genetic loci for childhood BMI and 18 for childhood obesity, the majority of which overlap 78 , 79 . There is also a clear overlap with genetic loci identified in adults, for example for FTO , MC4R and TMEM18 , but this overlap is not complete, some loci are specific to early life BMI, or have a relatively larger contribution in childhood 78 , 79 , 80 . These findings suggest that biological mechanisms underlying obesity in childhood are mostly similar to those in adulthood, but the relative influence of these mechanisms may differ at different phases of life.
The role of epigenetic processes in childhood and adolescent obesity has gained increasing attention. In children, several studies found associations between DNA methylation and BMI 81 , 82 , 83 , 84 , but a meta-analysis including data from >4,000 children identified only minimal associations 85 . Most studies support the hypothesis that DNA methylation changes are predominantly a consequence rather than a cause of obesity, which may explain the lower number of identified (up to 12) associations in children, in whom duration of exposure to a higher BMI is shorter than in adults, in whom associations with DNA methylation at hundreds of sites have been identified 85 , 86 , 87 . In addition to DNA methylation, some specific circulating microRNAs have been found to be associated with obesity in childhood 84 .
The field of epigenetic studies in childhood obesity is relatively young and evolving quickly. Future studies will need to focus on defining robust associations in blood as well as other tissues and on identifying cause-and-effect relationships. In addition, other omics, such as metabolomics and proteomics, are promising areas that may contribute to an improved aetiological understanding or may provide biological signatures that can be used as predictive or prognostic markers of childhood obesity and its comorbidities.
Parental obesity and childhood obesity
There is an established link between increased parental BMI and increased childhood BMI 88 , 89 . This link may be due to shared genetics, shared environment, a direct intrauterine effect of maternal BMI or a combination of these factors. In the case of shared genetics, the child inherits BMI-increasing genetic variants from one or both parents. Shared environmental factors, such as diet or lifestyle, may also contribute to an increased BMI in both parents and child. In addition, maternal obesity might create an intrauterine environment that programmes metabolic processes in the fetus, which increases the risk of childhood obesity. Some studies show larger effects of maternal than paternal BMI, indicating a potential causal intrauterine mechanism of maternal obesity, but evidence showing similar maternal and paternal effects is increasing. The data may indicate that there is only a limited direct intrauterine effect of maternal obesity on childhood obesity; rather, genetic effects inherited from the mother or father, or both, and/or shared environmental factors may contribute to childhood obesity risk 90 , 91 , 92 , 93 , 94 , 95 .
Diagnosis, screening and prevention
Diagnostic work-up.
The extent of overweight in clinical practice is estimated using BMI based on national charts 96 , 97 , 98 , 99 , 100 . Of note, the clinical classification of overweight or obesity differ depending on the BMI charts used and national recommendations; hence, local guidelines should be referred to. For example, the US CDC Growth Charts and several others use the 85th and 95th centile cut-points to denote overweight and obesity, respectively 19 . The WHO Growth Reference for children aged 5–19 years defines cut-points for overweight and obesity as a BMI-for-age greater than +1 and +2 SDs for BMI for age, respectively 18 . For children <5 years of age, overweight and obesity are defined as weight-for-height greater than +2 and +3 SDs, respectively, above the WHO Child Growth Standards median 17 . The IOTF and many countries in Europe use cut-points of 85th, 90th and 97th to define overweight, obesity and extreme obesity 26 .
BMI as an indirect measurement of body fat has some limitations; for example, pronounced muscle tissue leads to an increase in BMI, and BMI is not independent of height. In addition, people of different ethnicities may have different cut-points for obesity risk; for example, cardiometabolic risk occurs at lower BMI values in individuals with south Asian than in those with European ancestry 101 . Thus, BMI is best seen as a convenient screening tool that is supplemented by clinical assessment and investigations.
Other measures of body fat may help differentiate between fat mass and other tissues. Some of these tools are prone to low reliability, such as body impedance analyses (high day-to-day variation and dependent on level of fluid consumption) or skinfold thickness (high inter-observer variation), or are more expensive or invasive, such as MRI, CT or dual-energy X-ray absorptiometry, than simpler measures of body composition or BMI assessment.
Primary diseases rarely cause obesity in children and adolescents (<2%) 102 . However, treatable diseases should be excluded in those with obesity. A suggested diagnostic work-up is summarized in Fig. 4 . Routine measurement of thyroid-stimulating hormone (TSH) is not recommended 96 . Moderately elevated TSH levels (usually <10 IU/l) are frequently observed in obesity and are a consequence, and not a cause, of obesity 103 . In a growing child with normal height velocity, a normal BMI at the age of 2 years and normal cognitive development, no further diagnostic steps are necessary to exclude primary diseases 96 , 104 .

Concerning findings from a detailed medical history and physical examination will lead to further examinations. In individuals with early onset, extreme obesity (before age 3 years) and signs of hyperphagia, serum leptin level should be measured to rule out the extremely rare condition of congenital leptin deficiency. In individuals with normal or high leptin levels, genetic testing is indicated to search for monogenetic obesity. In individuals with intellectual disability, a syndromic disease may be present. Signs of impaired growth velocity or the history of central nervous system trauma or surgery will result in deeper endocrine evaluation and/or brain MRI. BDNF , brain-derived neurotropic factor; FT4, free thyroxin; KSR2 , kinase suppressor of ras 2; MC4R , melanocortin 4 receptor; POMC , pro-opiomelanocortin; SH2B1 , Src-homology 2 (SH2) B adapter protein 1; SIM1 , single-minded homologue 1; TSH, thyroid-stimulating hormone.
Clinical findings which need no further examination include pseudogynaecomastia (adipose tissue mimicking breast development; differentiated from breast tissue by ultrasonography), striae (caused by rapid weight increase) and a hidden penis in suprapubic adipose tissue (differentiated from micropenis by measurement of stretched penis length while pressing down on the suprapubic adipose tissue) 96 , 105 . Girls with obesity tend to have an earlier puberty onset (usually at around 8–9 years of age) and boys with severe obesity may have a delayed puberty onset (usually at around 13–14 years of age) 106 . Thus, if pubertal onset is slightly premature in girls or slightly delayed in boys, no further endocrine assessment is necessary.
Assessment of obesity-associated comorbidities
A waist to height ratio of >0.5 is a simple tool to identify central obesity 107 , 108 . Screening for cardiometabolic risk factors and fatty liver disease is recommended, especially in adolescents, and in those with more severe obesity or central adiposity, a strong family history of T2DM or premature heart disease, or relevant clinical symptoms, such as high blood pressure or acanthosis nigricans 96 , 97 , 98 , 99 , 109 . Investigations generally include fasting glucose levels, lipid profile, liver function and glycated haemoglobin, and might include an oral glucose tolerance test, polysomnography, and additional endocrine tests for polycystic ovary syndrome 96 , 97 , 98 , 99 .
T2DM in children and adolescents often occurs in the presence of a strong family history and may not be related to obesity severity 110 . T2DM onset usually occurs during puberty, a physiological state associated with increased insulin resistance 111 and, therefore, screening for T2DM should be considered in children and adolescents with obesity and at least one risk factor (family history of T2DM or features of metabolic syndrome) starting at pubertal onset 112 . As maturity-onset diabetes of the young (MODY) type II and type III are more frequent than T2DM in children and adolescents in many ethnicities, genetic screening for MODY may be appropriate 112 . Furthermore, type 1 diabetes mellitus (T1DM) should be excluded by measurement of autoantibodies in any individual with suspected diabetes with obesity. The differentiation of T2DM from MODY and T1DM is important as the diabetes treatment approaches differ 112 .
Several comorbidities of obesity should be considered if specific symptoms occur 96 , 109 . For polycystic ovary syndrome in hirsute adolescent girls with oligomenorrhoea or amenorrhoea, moderately increased testosterone levels and decreased sex hormone binding globulin levels are typical laboratory findings 113 . Obstructive sleep apnoea can occur in those with more severe obesity and who snore, have daytime somnolence or witnessed apnoeas. Diagnosis is made by polysomnography 114 . Minor orthopaedic disorders, such as flat feet and genu valgum, are frequent in children and adolescents with obesity and may cause pain. Major orthopaedic complications include slipped capital femoral epiphyses (acute and chronic), which manifest with hip and knee pain in young adolescents and are characterized by reduced range of hip rotation and waddling gait; and Blount disease (tibia vara), typically occurring in children aged 2–5 years 105 , 115 . In addition, children and adolescents with extreme obesity frequently have increased dyspnoea and decreased exercise capacity. A heightened demand for ventilation, elevated work of breathing, respiratory muscle inefficiency and diminished respiratory compliance are caused by increased truncal fat mass. This may result in a decreased functional residual capacity and expiratory reserve volume, ventilation to perfusion ratio abnormalities and hypoxaemia, especially when supine. However, conventional respiratory function tests are only mildly affected by obesity except in extreme cases 116 . Furthermore, gallstones should be suspected in the context of abdominal pain after rapid weight loss, which can be readily diagnosed via abdominal ultrasonography 105 . Finally, pseudotumor cerebri may present with chronic headache, and depression may present with flat affect, chronic fatigue and sleep problems 105 .
Obesity in adolescents can also be associated with disordered eating, eating disorders and other psychological disorders 117 , 118 . If suspected, assessment by a mental health professional is recommended.
A comprehensive approach
The 2016 report of the WHO Commission on Ending Childhood Obesity stated that progress in tackling childhood obesity has been slow and inconsistent, with obesity prevention requiring a whole-of-government approach in which policies across all sectors systematically take health into account, avoiding harmful health impacts and, therefore, improving population health and health equity 13 , 119 . The focus in developing and implementing interventions to prevent obesity in children should be on interventions that are feasible, effective and likely to reduce health inequalities 14 . Importantly, the voices of children and adolescents living with social disadvantage and those from minority groups must be heard if such interventions are to be effective and reduce inequalities 120 .
Figure 5 presents a system for the prevention of childhood obesity within different domains of the socioecological model 121 and highlights opportunities for interventions. These domains can be described on a continuum, from (most downstream) individual and interpersonal (including parents, peers and wider family) through to organizational (including health care and schools), community (including food, activity and environment), society (including media and finally cultural norms) and (most upstream) public policy (from local to national level). Interventions to prevent childhood obesity can be classified on the Nuffield intervention ladder 122 . This framework was proposed by the Nuffield Council on Bioethics in 2007 (ref. 122 ) and distributes interventions on the ladder steps depending on the degree of agency required by the individual to make the behavioural changes that are the aim of the intervention. The bottom step of the ladder includes interventions that provide information, which requires the highest agency and relies on a child, adolescent and/or family choosing (and their ability to choose) to act on that information and change behaviour. The next steps of the ladder are interventions that enable choice, guide choice through changing the default policy, guide choice through incentives, guide choice through disincentives, or restrict choice. On the top-most step of the ladder (lowest agency required) are interventions that eliminate choice.

This schematic integrates interventions that were included in a Cochrane review 127 of 153 randomized controlled trials of interventions to prevent obesity in children and are high on the Nuffield intervention ladder 122 . The Nuffield intervention ladder distributes interventions depending on the degree of agency required for the behavioural changes that are the aim of the intervention. The socioecological model 121 comprises different domains (or levels) from the individual up to public policy. Interventions targeting the individual and interpersonal domains can be described as downstream interventions, and interventions within public policy can be described as the highest level of upstream interventions. Within each of these domains, arrow symbols with colours corresponding to the Nuffield intervention ladder category are used to show interventions that were both included in the Cochrane review 127 and that guide, restrict or eliminate choice as defined by the Nuffield intervention ladder 122 . Upstream interventions, and interventions on the top steps of the Nuffield ladder, are more likely to reduce inequalities. NGO, non-governmental organization.
Downstream and high-agency interventions (on the bottom steps of the Nuffield ladder) are more likely to result in intervention-generated inequalities 123 . This has been elegantly described and evidenced, with examples from the obesity prevention literature 124 , 125 . A particularly strong example is a systematic review of 38 interventions to promote healthy eating that showed that food price (an upstream and low-agency intervention) seemed to decrease inequalities, all interventions that combined taxes and subsidies consistently decreased inequalities, and downstream high-agency interventions, especially dietary counselling, seemed to increase inequalities 126 .
Effectiveness of prevention interventions
A 2019 Cochrane review of interventions to prevent obesity in children 127 included 153 randomized controlled trials (RCTs), mainly in HICs (12% were from middle-income countries). Of these RCTs, 56% tested interventions in children aged 6–12 years, 24% in children aged 0–5 years, and 20% in adolescents aged 13–18 years. The review showed that diet-only interventions to prevent obesity in children were generally ineffective across all ages. Interventions combining diet and physical activity resulted in modest benefits in children aged 0–12 years but not in adolescents. However, physical activity-only interventions to prevent obesity were effective in school-age children (aged 5–18 years). Whether the interventions were likely to work equitably in all children was investigated in 13 RCTs. These RCTs did not indicate that the strategies increased inequalities, although most of the 13 RCTs included relatively homogeneous groups of children from disadvantaged backgrounds.
The potential for negative unintended consequences of obesity prevention interventions has received much attention 128 . The Cochrane review 127 investigated whether children were harmed by any of the strategies; for example, by having injuries, losing too much weight or developing damaging views about themselves and their weight. Of the few RCTs that did monitor these outcomes, none found any harms in participants.
Intervention levels
Most interventions (58%) of RCTs in the Cochrane review aimed to change individual lifestyle factors via education-based approaches (that is, simply provide information) 129 . In relation to the socioecological model, only 11 RCTs were set in the food and physical activity environment domain, and child care, preschools and schools were the most common targets for interventions. Of note, no RCTs were conducted in a faith-based setting 130 . Table 2 highlights examples of upstream interventions that involve more than simply providing information and their classification on the Nuffield intervention ladder.
Different settings for interventions to prevent childhood obesity, including preschools and schools, primary health care, community settings and national policy, offer different opportunities for reach and effectiveness, and a reduction in inequalities.
Preschools and schools are key settings for public policy interventions for childhood obesity prevention, and mandatory and voluntary food standards and guidance on physical education are in place in many countries. Individual schools are tasked with translating and implementing these standards and guidance for their local context. Successful implementation of a whole-school approach, such as that used in the WHO Nutrition-Friendly Schools Initiative 131 , is a key factor in the effectiveness of interventions. Careful consideration should be given to how school culture can, and needs to, be shifted by working with schools to tailor the approach and manage possible staff capacity issues, and by building relationships within and outside the school gates to enhance sustainability 132 , 133 .
Primary health care offers opportunities for guidance for obesity prevention, especially from early childhood to puberty. Parent-targeted interventions conducted by clinicians in health-care or community settings have the strongest level of evidence for their effectiveness in reducing BMI z -score at age 2 years 134 . These interventions include group programmes, clinic nurse consultations, mobile phone text support or nurse home visiting, and focusing on healthy infant feeding, healthy childhood feeding behaviours and screen time.
A prospective individual participant data meta-analysis of four RCTs involving 2,196 mother–baby dyads, and involving nurse home visiting or group programmes, resulted in a small but significant reduction in BMI in infants in the intervention groups compared with control infants at age 18–24 months 134 . Improvements were also seen in television viewing time, breastfeeding duration and feeding practices. Interventions were more effective in settings with limited provision of maternal and child health services in the community. However, effectiveness diminished by age 5 years without further intervention, highlighting the need for ongoing interventions at each life stage 135 . Evidence exists that short-duration interventions targeting sleep in very early childhood may be more effective than nutrition-targeted interventions in influencing child BMI at age 5 years 136 .
Primary care clinicians can provide anticipatory guidance, as a form of primary prevention, to older children, adolescents and their families, aiming to support healthy weight and weight-related behaviours. Clinical guidelines recommend that clinicians monitor growth regularly, and provide guidance on healthy eating patterns, physical activity, sedentary behaviours and sleep patterns 97 , 100 . Very few paediatric trials have investigated whether this opportunistic screening and advice is effective in obesity prevention 100 . A 2021 review of registered RCTs for the prevention of obesity in infancy found 29 trials 137 , of which most were delivered, or were planned to be delivered, in community health-care settings, such as nurse-led clinics. At the time of publication, 11 trials had reported child weight-related outcomes, two of which showed a small but significant beneficial effect on BMI at age 2 years, and one found significant improvements in the prevalence of obesity but not BMI. Many of the trials showed improvements in practices, such as breastfeeding and screen time.
At the community level, local public policy should be mindful of the geography of the area (such as urban or rural) and population demographics. Adolescents usually have more freedom in food and beverage choices made outside the home than younger children. In addition, physical activity levels usually decline and sedentary behaviours rise during adolescence, particularly in girls 138 , 139 . These behavioural changes offer both opportunities and barriers for those developing community interventions. On a national societal level, public policies for interventions to prevent obesity in children include the control of advertising of foods and beverages high in fat, sugar and/or salt in some countries. Industry and the media, including social media, can have a considerable influence on the food and physical activity behaviours of children 13 , 119 .
Public policy may target interventions at all domains from the individual to the societal level. The main focus of interventions in most national public policies relies on the ability of individuals to make the behavioural changes that are the aim of the intervention (high-agency interventions) at the individual level (downstream interventions). An equal focus on low-agency and upstream interventions is required if a step change in tackling childhood obesity is to be realized 140 , 141 .
COVID-19 and obesity
Early indications in several countries show rising levels of childhood obesity, and an increase in inequalities in childhood obesity during the COVID-19 pandemic 142 . The substantial disruptions in nutrition and lifestyle habits of children during and since the pandemic include social isolation and addiction to screens 143 . Under-nutrition is expected to worsen in poor countries, but obesity rates could increase in middle-income countries and HICs, especially among vulnerable groups, widening the gap in health and social inequalities 143 . Public health approaches at national, regional and local levels should include strategies that not only prevent obesity and under-nutrition, but also reduce health inequalities.
In summary, although most trials of obesity prevention have occurred at the level of the individual, the immediate family, school or community, effective prevention of obesity will require greater investment in upstream, low-agency interventions.
Treatment goals
Treatment should be centred on the individual and stigma-free (Box 1 ) and may aim for a reduction in overweight and improvement in associated comorbidities and health behaviours. Clinical considerations when determining a treatment approach should include age, severity of overweight and the presence of associated complications 144 , 145 .
Box 1 Strategies for minimizing weight stigma in health care 220 , 221 , 222
Minimizing weight bias in the education of health-care professionals
Improved education of health professionals:
pay attention to the implicit and explicit communication of social norms
include coverage of the broader determinants of obesity
include discussion of harms caused by social and cultural norms and messages concerning body weight
provide opportunities to practise non-stigmatizing care throughout education
Provide causal information focusing on the genetic and/or socioenvironmental determinants of weight.
Provide empathy-invoking interventions, emphasizing size acceptance, respect and human dignity.
Provide a weight-inclusive approach, by emphasizing that all individuals, regardless of size, have the right to equal health care.
Addressing health facility infrastructure and processes
Provide appropriately sized chairs, blood pressure cuffs, weight scales, beds, toilets, showers and gowns.
Use non-stigmatizing language in signage, descriptions of clinical services and other documentation.
Providing clinical leadership and using appropriate language within health-care settings
Senior clinicians and managers should role-model supportive and non-biased behaviours towards people with obesity and indicate that they do not tolerate weight-based discrimination in any form.
Staff should identify the language that individuals prefer in referring to obesity.
Use person-first language, for example a ‘person with obesity’ rather than ‘an obese person’.
Treatment guidelines
Clinical guidelines advise that first-line management incorporates a family-based multicomponent approach that addresses dietary, physical activity, sedentary and sleep behaviours 97 , 99 , 109 , 146 . This approach is foundational, with adjunctive therapies, especially pharmacotherapy and bariatric surgery, indicated under specific circumstances, usually in adolescents with more severe obesity 144 , 145 . Guideline recommendations vary greatly among countries and are influenced by current evidence, and functionality and resourcing of local health systems. Hence, availability and feasibility of therapies differs internationally. In usual clinical practice, interventions may have poorer outcomes than is observed in original studies or anticipated in evidence-based guidelines 147 because implementation of guidelines is more challenging in resource-constrained environments 148 . In addition, clinical trials are less likely to include patients with specialized needs, such as children from culturally diverse populations, those living with social disadvantage, children with complex health problems, and those with severe obesity 149 , 150 .
Behavioural interventions
There are marked differences in individual responses to behavioural interventions, and overall weight change outcomes are often modest. In children aged 6–11 years, a 2017 Cochrane review 150 found that mean BMI z -scores were reduced in those involved in behaviour-changing interventions compared with those receiving usual care or no treatment by only 0.06 units (37 trials; 4,019 participants; low-quality evidence) at the latest follow-up (median 10 months after the end of active intervention). In adolescents aged 12–17 years, another 2017 Cochrane review 149 found that multicomponent behavioural interventions resulted in a mean reduction in weight of 3.67 kg (20 trials; 1,993 participants) and reduction in BMI of 1.18 kg/m 2 (28 trials; 2,774 participants). These effects were maintained at the 24-month follow-up. A 2012 systematic review found significant improvements in LDL cholesterol triglycerides and blood pressure up to 1 year from baseline following lifestyle interventions in children and adolescents 151 .
Family-based behavioural interventions are recommended in national level clinical practice guidelines 97 , 100 , 146 , 152 . They are an important element of intensive health behaviour and lifestyle treatments (IHBLTs) 109 . Family-based approaches use behavioural techniques, such as goal setting, parental monitoring or modelling, taught in family sessions or in individual sessions separately to children and care givers, depending on the child’s developmental level. The priority is to encourage the whole family to engage in healthier behaviours that result in dietary improvement, greater physical activity, and less sedentariness. This includes making changes to the family food environment and requires parental monitoring.
Family-based interventions differ in philosophy and implementation from those based on family systems theory and therapy 153 . All are intensive interventions that require multiple contact hours (26 or more) with trained specialists delivered over an extended period of time (6–12 months) 10 . Changing family lifestyle habits is challenging and expensive, and the therapeutic expertise is not widely available. Moving interventions to primary care settings, delivered by trained health coaches, and supplemented by remote contact (for example by phone), will improve access and equity 154 .
Very few interventions use single psychological approaches. Most effective IHBLTs are multicomponent and intensive (many sessions), and include face-to-face contact. There has been interest in motivational interviewing as an approach to delivery 155 . As client-centred counselling, this places the young person at the centre of their behaviour change. Fundamental to motivational interviewing is the practitioner partnership that helps the young person and/or parents to explore ambivalence to change, consolidate commitment to change, and develop a plan based on their own insights and expertise. Evidence reviews generally support the view that motivational interviewing reduces BMI. Longer interventions (>4 months), those that assess and report on intervention fidelity, and those that target both diet and physical activity are most effective 155 , 156 .
More intensive dietary interventions
Some individuals benefit from more intensive interventions 98 , 144 , 157 , 158 , which include very low-energy diets, very low-carbohydrate diets and intermittent energy restriction 159 . These interventions usually aim for weight loss and are only recommended for adolescents who have reached their final height. These diets are not recommended for long periods of time due to challenges in achieving nutritional adequacy 158 , 160 , and lack of long-term safety data 158 , 161 . However, intensive dietary interventions may be considered when conventional treatment is unsuccessful, or when adolescents with comorbidities or severe obesity require rapid or substantial weight loss 98 . A 2019 systematic review of very low-energy diets in children and adolescents found a mean reduction in body weight of −5.3 kg (seven studies) at the latest follow‐up, ranging from 5 to 14.5 months from baseline 161 .
Pharmacological treatment
Until the early 2020s the only drug approved in many jurisdictions for the treatment of obesity in adolescents was orlistat, a gastrointestinal lipase inhibitor resulting in reduced uptake of lipids and, thereby, a reduced total energy intake 162 . However, the modest effect on weight in combination with gastrointestinal adverse effects limit its usefulness overall 163 .
A new generation of drugs has been developed for the treatment of both T2DM and obesity. These drugs are based on gastrointestinal peptides with effects both locally and in the central nervous system. GLP1 is an incretin that reduces appetite and slows gastric motility. The GLP1 receptor agonist liraglutide is approved for the treatment of obesity in those aged 12 years and older both in the USA and Europe 164 , 165 . Liraglutide, delivered subcutaneously daily at a higher dose than used for T2DM resulted in a 5% better BMI reduction than placebo after 12 months 166 . A 2022 trial of semaglutide, another GLP1 receptor agonist, delivered subcutaneously weekly in adolescents demonstrated 16% weight loss after 68 weeks of treatment, with modest adverse events and a low drop-out rate 12 . Tirzepatide, an agonist of both GLP1 and glucose-dependent insulinotropic polypeptide (GIP), is approved by the FDA for the treatment of T2DM in adults 167 . Subcutaneous tirzepatide weekly in adults with obesity resulted in ~20% weight loss over 72 weeks 168 . Of note, GIP alone increases appetite, but the complex receptor–agonist interaction results in downregulation of the GIP receptors 169 , illustrating why slightly modified agonists exert different effects. A study of the use of tirzepatide in adolescents with T2DM has been initiated but results are not expected before 2027 (ref. 170 ). No trials of tirzepatide are currently underway in adolescents with obesity but without T2DM.
Hypothalamic obesity is difficult to treat. Setmelanotide is a MC4R agonist that reduces weight and improves quality of life in most people with LEPR and POMC mutations 71 . In trials of setmelanotide, 8 of 10 participants with POMC deficiency and 5 of 11 with LEPR deficiency had weight loss of at least 10% at ~1 year. The mean percentage change in most hunger score from baseline was −27.1% and −43.7% in those with POMC deficiency and leptin receptor deficiency, respectively 71 .
In the near future, effective new drugs with, hopefully, an acceptable safety profile will be available that will change the way we treat and set goals for paediatric obesity treatment 171 .
Bariatric surgery
Bariatric surgery is the most potent treatment for obesity in adolescents with severe obesity. The types of surgery most frequently used are sleeve gastrectomy and gastric bypass, both of which reduce appetite 172 . Mechanisms of action are complex, involving changes in gastrointestinal hormones, neural signalling, bile acid metabolism and gut microbiota 173 . Sleeve gastrectomy is a more straightforward procedure and the need for vitamin supplementation is lower than with gastric bypass. However, long-term weight loss may be greater after gastric bypass surgery 174 .
Prospective long-term studies demonstrate beneficial effects of both sleeve gastrectomy and gastric bypass on weight loss and comorbidities in adolescents with severe obesity 175 , 176 . In a 5-year follow-up period, in 161 participants in the US TEEN-LABS study who underwent gastric bypass, mean BMI declined from 50 to 37 kg/m 2 (ref. 11 ). In a Swedish prospective study in 81 adolescents who underwent gastric bypass, the mean decrease in BMI at 5 years was 13.1 kg/m 2 (baseline BMI 45.5 kg/m 2 ) compared with a BMI increase of 3.1 kg/m 2 in the control group 176 . Both studies showed marked inter-individual variations. Negative adverse effects, including gastrointestinal problems, vitamin deficits and reduction in lean body mass, are similar in adults and adolescents. Most surgical complications following bariatric surgery in the paediatric population are minor, occurring in the early postoperative time frame, but 8% of patients may have major perioperative complications 177 . Up to one-quarter of patients may require subsequent related procedures within 5 years 109 . However, many adolescents with severe obesity also have social and psychological problems, highlighting the need for routine and long-term monitoring 109 , 178 .
Recommendations for bariatric surgery in adolescents differ considerably among countries, with information on long-term outcomes emerging rapidly. In many countries, bariatric surgery is recommended only from Tanner pubertal stage 3–4 and beyond, and only in children with severe obesity and cardiometabolic comorbidities 177 . The 2023 American Academy of Pediatrics clinical practice guidelines recommend that bariatric surgery be considered in adolescents ≥13 years of age with a BMI of ≥35 kg/m 2 or 120% of the 95th percentile for age and sex, whichever is lower, as well as clinically significant disease, such as T2DM, non-alcoholic fatty liver disease, major orthopaedic complications, obstructive sleep apnoea, the presence of cardiometabolic risk, or depressed quality of life 109 . For those with a BMI of ≥40 kg/m 2 or 140% of the 95th percentile for age and sex, bariatric surgery is indicated regardless of the presence of comorbidities. Potential contraindications to surgery include correctable causes of obesity, pregnancy and ongoing substance use disorder. The guidelines comment that further evaluation, undertaken by multidisciplinary centres that offer bariatric surgery for adolescents, should determine the capacity of the patient and family to understand the risks and benefits of surgery and to adhere to the required lifestyle changes before and after surgery.
Long-term weight outcomes
Few paediatric studies have investigated long-term weight maintenance after the initial, more intensive, weight loss phase. A 2018 systematic review of 11 studies in children and adolescents showed that a diverse range of maintenance interventions, including support via face-to-face psychobehavioural therapies, individual physician consultations, or adjunctive therapeutic contact via newsletters, mobile phone text or e-mail, led to stabilization of BMI z -score compared with control participants, who had increases in BMI z -score 179 . Interventions that are web-based or use mobile devices may be particularly useful in young people 180 .
One concern is weight regain which occurs after bariatric surgery in general 181 but may be more prevalent in adolescents 176 . For example, in a Swedish prospective study, after 5 years, 25–30% of participants fulfilled the definitions of low surgical treatment effectiveness, which was associated with poorer metabolic outcomes 176 . As with adults, prevention of weight regain for most at-risk individuals might be possible with the combination of lifestyle support and pharmacological treatment 182 . Further weight maintenance strategies and long-term outcomes are discussed in the 2023 American Academy of Pediatrics clinical practice guidelines 109 . The appropriate role and timing of other therapies for long-term weight loss maintenance, such as anti-obesity medications, more intensive dietary interventions and bariatric surgery, are areas for future research.
In summary, management of obesity in childhood and adolescence requires intensive interventions. Emerging pharmacological therapies demonstrate greater short-term effectiveness than behavioural interventions; however, long-term outcomes at ≥2 years remain an important area for future research.
Quality of life
Weight bias describes the negative attitudes to, beliefs about and behaviour towards people with obesity 183 . It can lead to stigma causing exclusion, and discrimination in work, school and health care, and contributes to the inequities common in people with obesity 184 . Weight bias also affects social engagement and psychological well-being of children.
Children and adolescents with obesity score lower overall on health-related quality of life (HRQoL) 4 , 5 . In measures that assess domains of functioning, most score lower in physical functioning, physical/general health and psychosocial areas, such as appearance, and social acceptance and functioning. HRQoL is lowest in treatment-seeking children and in those with more extreme obesity 185 . Weight loss interventions generally increase HRQoL independent of the extent of weight loss 186 , especially in the domains most affected. However, changes in weight and HRQoL are often not strongly correlated. This may reflect a lag in the physical and/or psychosocial benefit from weight change, or the extent of change that is needed to drive change in a child’s self-perception.
Similar observations apply to the literature on self-esteem. Global self-worth is reduced in children and adolescents with obesity, as is satisfaction with physical appearance, athletic competence and social acceptance 187 . Data from intensive interventions suggest the psychological benefit of weight loss may be as dependent on some feature of the treatment environment or supportive social network as the weight loss itself 188 . This may include the daily company of others with obesity, making new friendships, and experienced improvements in newly prioritized competences.
There is a bidirectional relationship between HRQoL and obesity 189 , something also accepted in the relationship with mood disorder. Obesity increases the risk of depression and vice versa, albeit over a longer period of time and which may only become apparent in adulthood 190 . Obesity also presents an increased risk of anxiety 191 .
Structured and professionally delivered weight management interventions ameliorate mood disorder symptoms 192 and improve self-esteem 193 . Regular and extended support are important components beyond losing weight. Such interventions do not increase the risk of eating disorders 194 . This is despite a recognition that binge eating disorder is present in up to 5% of adolescents with overweight or obesity 195 . They are five times more likely to have binge eating symptoms than those with average weight. Importantly, adolescents who do not have access to professionally delivered weight management may be more likely to engage in self-directed dieting, which is implicated in eating disorder development 196 .
The literature linking childhood obesity with either attention deficit hyperactivity disorder or autism spectrum disorder is complex and the relationship is uncertain. The association seems to be clearer in adults but the mechanisms and their causal directions remain unclear 109 , 197 . Young children with obesity, especially boys, are more likely to be parent-rated as having behavioural problems 198 . This may be a response to the behaviour of others rather than reflect clinical diagnoses such as attention deficit hyperactivity disorder or autism spectrum disorder. Conduct and peer relationship problems co-occur in children, regardless of their weight.
Children with obesity experience more social rejection. They receive fewer friendship nominations and more peer rejections, most pronounced in those with severe obesity 199 . This continues through adolescence and beyond. Children with obesity are more likely to report being victimized 200 . Younger children may respond by being perpetrators themselves. While it is assumed that children are victimized because of their weight, very few studies have looked at the nature or reason behind victimization. A substantial proportion of children with obesity fail to identify themselves as being fat-teased 187 . Although the stigma associated with obesity should be anticipated in children, especially in those most overweight, it would be inappropriate to see all as victims. A better understanding of children’s resilience is needed.
Many gaps remain in basic, translational and clinical research in child and adolescent obesity. The mechanisms (genetic, epigenetic, environmental and social) behind the overwhelming association between parental obesity and child and adolescent obesity are still unclear given the paradoxically weak association in BMI between adopted children and their parents in combination with the modest effect size of known genetic loci associated with obesity 201 .
Early manifestation of extreme obesity in childhood suggests a strong biological basis for disturbances of homeostatic weight regulation. Deep genotyping (including next-generation sequencing) and epigenetic analyses in these patients will reveal new genetic causes and causal pathways as a basis for the development of mechanism-based treatments. Future work aiming to understand the mechanisms underlying the development of childhood obesity should consider the complex biopsychosocial interactions and take a systems approach to understanding causal pathways leading to childhood obesity to contribute to evidence-based prevention and treatment strategies.
Long-term outcome data to better determine the risks of eating disorders are required. Although symptoms improve during obesity treatment in most adolescents, screening and monitoring for disordered eating is recommended in those presenting for treatment 202 and effective tools for use in clinical practice are required. A limited number of tools are validated to identify binge eating disorder in youth with obesity 203 but further research is needed to screen appropriately for the full spectrum of eating disorder diagnoses in obesity treatment seeking youth 203 . Recent reviews provide additional detail regarding eating disorder risk in child and adolescent obesity 117 , 202 , 204 .
Most studies of paediatric obesity treatment have been undertaken in HICs and predominantly middle-class populations. However, research is needed to determine which strategies are best suited for those in LMICs and low-resource settings, for priority population groups including indigenous peoples, migrant populations and those living with social disadvantage, and for children with neurobehavioural and psychiatric disorders. We currently have a limited understanding of how best to target treatment pathways for different levels of genetic risk, age, developmental level, obesity severity, and cardiometabolic and psychological risk. Current outcomes for behavioural interventions are relatively modest and improved treatment outcomes are needed to address the potentially severe long-term health outcomes of paediatric obesity. Studies also need to include longer follow-up periods after an intervention, record all adverse events, incorporate cost-effectiveness analyses and have improved process evaluation.
Other areas in need of research include the role of new anti-obesity medications especially in adolescents, long-term outcomes following bariatric surgery and implementation of digital support systems to optimize outcomes and reduce costs of behavioural change interventions 205 . We must also better understand and tackle the barriers to implementation of treatment in real-life clinical settings, including the role of training of health professionals. Importantly, treatment studies of all kinds must engage people with lived experience — adolescents, parents and families — to understand what outcomes and elements of treatment are most valued.
Obesity prevention is challenging because it requires a multilevel, multisectoral approach that addresses inequity, involves many stakeholders and addresses both the upstream and the downstream factors influencing obesity risk. Some evidence exists of effectiveness of prevention interventions operating at the level of the child, family and school, but the very poor progress overall in modifying obesity prevalence globally highlights many areas in need of research and evidence implementation. Studies are needed especially in LMICs, particularly in the context of the nutrition transition and the double burden of malnutrition. A focus on intergenerational research, rather than the age-based focus of current work, is also needed. Systems research approaches should be used, addressing the broader food and physical activity environments, and links to climate change 206 . In all studies, strategies are needed that enable co-production with relevant communities, long-term follow-up, process evaluation and cost-effectiveness analyses. In the next few years, research and practice priorities must include a focus on intervention strategies in the earliest phases of life, including during pregnancy. The effects of COVID-19 and cost of living crises in many countries are leading to widening health inequalities 207 and this will further challenge obesity prevention interventions. Available resourcing for prevention interventions may become further constrained, requiring innovative solutions across agendas, with clear identification of co-benefits. For example, public health interventions for other diseases, such as dental caries or depression, or other societal concerns, such as urban congestion or climate change, may also act as obesity prevention strategies. Ultimately, to implement obesity prevention, societal changes are needed in terms of urban planning, social structures and health-care access.
Future high-quality paediatric obesity research can be enabled through strategies that support data sharing, which avoids research waste and bias, and enables new research questions to be addressed. Such approaches require leadership, careful engagement of multiple research teams, and resourcing. Four national or regional level paediatric weight registries exist 208 , 209 , 210 , 211 , which are all based in North America or Europe. Such registries should be established in other countries, especially in low-resource settings, even if challenging 208 . Another data-sharing approach is through individual participant data meta-analyses of intervention trials, which can include prospectively collected data 212 and are quite distinct from systematic reviews of aggregate data. Two recent examples are the Transforming Obesity Prevention in Childhood (TOPCHILD) Collaboration, which includes early interventions to prevent obesity in the first 2 years of life 213 , and the Eating Disorders in Weight-Related Therapy (EDIT) Collaboration, which aims to identify characteristics of individuals or trials that increase or protect against eating disorder risk following obesity treatment 214 . Formal data linkage studies, especially those joining up routine administrative datasets, enable longer-term and broader outcome measures to be assessed than is possible with standard clinical or public health intervention studies.
Collaborative research will also be enhanced through the use of agreed core outcome sets, supporting data harmonization. The Edmonton Obesity Staging System – Paediatric 215 is one option for paediatric obesity treatment. A core outcome set for early intervention trials to prevent obesity in childhood (COS-EPOCH) has been recently established 216 . These efforts incorporate a balance between wanting and needing to share data and adhering to privacy protection regulations. Objective end points are ideal, including directly measured physical activity and body composition.
Collaborative efforts and a systems approach are paramount to understand, prevent and manage child and adolescent obesity. Research funding and health policies should focus on feasible, effective and equitable interventions.
NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet https://doi.org/10.1016/S0140-6736(17)32129-3 (2017).
Article Google Scholar
Popkin, B. M., Corvalan, C. & Grummer-Strawn, L. M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 395 , 65–74 (2020).
Article PubMed Google Scholar
Kompaniyets, L. et al. Underlying medical conditions associated with severe COVID-19 illness among children. JAMA Netw. Open 4 , e2111182 (2021).
Article PubMed PubMed Central Google Scholar
Griffiths, L. J., Parsons, T. J. & Hill, A. J. Self‐esteem and quality of life in obese children and adolescents: a systematic review. Int. J. Pediatr. Obes. 5 , 282–304 (2010).
Buttitta, M., Iliescu, C., Rousseau, A. & Guerrien, A. Quality of life in overweight and obese children and adolescents: a literature review. Qual. Life Res. 23 , 1117–1139 (2014).
Hayes, A. et al. Early childhood obesity: association with healthcare expenditure in Australia. Obesity 24 , 1752–1758 (2016).
Marcus, C., Danielsson, P. & Hagman, E. Pediatric obesity – long-term consequences and effect of weight loss. J. Intern. Med. 292 , 870–891 (2022).
Berthoud, H. R., Morrison, C. D. & Münzberg, H. The obesity epidemic in the face of homeostatic body weight regulation: what went wrong and how can it be fixed? Physiol. Behav. 222 , 112959 (2020).
Article CAS PubMed PubMed Central Google Scholar
World Health Organization. Report of the commission on ending childhood obesity. WHO https://www.who.int/publications/i/item/9789241510066 (2016). This report from the WHO on approaches to childhood and adolescent obesity has six main recommendations for governments, covering food and physical activity, age-based settings and provision of weight management for those with obesity.
O’Connor, E. A. et al. Screening for obesity and intervention for weight management in children and adolescents: evidence report and systematic review for the US Preventive Services Task Force. JAMA 317 , 2427–2444 (2017).
Inge, T. H. et al. Five-year outcomes of gastric bypass in adolescents as compared with adults. N. Engl. J. Med. 380 , 2136–2145 (2019).
Weghuber, D. et al. Once-weekly semaglutide in adolescents with obesity. N. Engl. J. Med. https://doi.org/10.1056/NEJMoa2208601 (2022). To our knowledge, the first RCT of semaglutide 2.4 mg, administered weekly by subcutaneous injection, in adolescents with obesity.
World Health Organization. Report of the Commission on Ending Childhood Obesity: Implementation Plan: Executive Summary (WHO, 2017).
Hillier-Brown, F. C. et al. A systematic review of the effectiveness of individual, community and societal level interventions at reducing socioeconomic inequalities in obesity amongst children. BMC Public Health 14 , 834 (2014).
World Health Organization. Obesity. WHO https://www.who.int/health-topics/obesity#tab=tab_1 (2023).
Mei, Z. et al. Validity of body mass index compared with other body-composition screening indexes for the assessment of body fatness in children and adolescents. Am. J. Clin. Nutr. 75 , 978–985 (2002).
Article CAS PubMed Google Scholar
World Health Organization. Child growth standards. WHO https://www.who.int/tools/child-growth-standards/standards (2006).
World Health Organization. Growth reference data for 5–19 years. WHO https://www.who.int/tools/growth-reference-data-for-5to19-years (2007).
National Center for Health Statistics. CDC growth charts. Centers for Disease Control and Prevention http://www.cdc.gov/growthcharts/ (2022).
Cole, T. J., Bellizzi, M. C., Flegal, K. M. & Dietz, W. H. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 320 , 1240 (2000).
Di Cesare, M. et al. The epidemiological burden of obesity in childhood: a worldwide epidemic requiring urgent action. BMC Med. 17 , 212 (2019).
Swinburn, B., Egger, G. & Raza, F. Dissecting obesogenic environments: the development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 29 , 563–570 (1999).
Ford, N. D., Patel, S. A. & Narayan, K. V. Obesity in low-and middle-income countries: burden, drivers, and emerging challenges. Annu. Rev. Public Health 38 , 145–164 (2017).
Shah, B., Tombeau Cost, K., Fuller, A., Birken, C. S. & Anderson, L. N. Sex and gender differences in childhood obesity: contributing to the research agenda. BMJ Nutr. Prev. Health 3 , 387–390 (2020).
Public Health England. Research and analysis: differences in child obesity by ethnic group. GOV.UK https://www.gov.uk/government/publications/differences-in-child-obesity-by-ethnic-group/differences-in-child-obesity-by-ethnic-group#data (2019).
Cole, T. J. & Lobstein, T. Extended international (IOTF) body mass index cut‐offs for thinness, overweight and obesity. Pediatr. Obes. 7 , 284–294 (2012).
Kelly, A. S. et al. Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches: a scientific statement from the American Heart Association. Circulation 128 , 1689–1712 (2013).
Garnett, S. P., Baur, L. A., Jones, A. M. & Hardy, L. L. Trends in the prevalence of morbid and severe obesity in Australian children aged 7–15 years, 1985-2012. PLoS ONE 11 , e0154879 (2016).
Spinelli, A. et al. Prevalence of severe obesity among primary school children in 21 European countries. Obes. Facts 12 , 244–258 (2019).
Twig, G. et al. Body-Mass Index in 2.3 million adolescents and cardiovascular death in adulthood. N. Engl. J. Med. 374 , 2430–2440 (2016).
González-Muniesa, P. et al. Obesity. Nat. Rev. Dis. Primers 3 , 17034 (2017).
Geserick, M. et al. Acceleration of BMI in early childhood and risk of sustained obesity. N. Engl. J. Med. 379 , 1303–1312 (2018).
Larqué, E. et al. From conception to infancy – early risk factors for childhood obesity. Nat. Rev. Endocrinol. 15 , 456–478 (2019).
Barker, D. J. Fetal origins of coronary heart disease. Br. Med. J. 311 , 171–174 (1995).
Article CAS Google Scholar
Gluckman, P. D., Hanson, M. A., Cooper, C. & Thornburg, K. L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 359 , 61–73 (2008).
Philips, E. M. et al. Changes in parental smoking during pregnancy and risks of adverse birth outcomes and childhood overweight in Europe and North America: an individual participant data meta-analysis of 229,000 singleton births. PLoS Med. 17 , e1003182 (2020).
Voerman, E. et al. Maternal body mass index, gestational weight gain, and the risk of overweight and obesity across childhood: an individual participant data meta-analysis. PLoS Med. 16 , e1002744 (2019). Individual participant data meta-analysis of >160,000 mothers and their children on the associations of maternal BMI and gestational weight gain and childhood overweight or obesity.
McIntyre, H. D. et al. Gestational diabetes mellitus. Nat. Rev. Dis. Primers 5 , 47 (2019).
Oken, E. & Gillman, M. W. Fetal origins of obesity. Obes. Res. 11 , 496–506 (2003).
Hughes, A. R., Sherriff, A., Ness, A. R. & Reilly, J. J. Timing of adiposity rebound and adiposity in adolescence. Pediatrics 134 , e1354–e1361 (2014).
Rolland-Cachera, M. F. et al. Tracking the development of adiposity from one month of age to adulthood. Ann. Hum. Biol. 14 , 219–229 (1987).
Koletzko, B. et al. Prevention of childhood obesity: a position paper of the Global Federation of International Societies of Paediatric Gastroenterology, Hepatology and Nutrition (FISPGHAN). J. Pediatr. Gastroenterol. Nutr. 70 , 702–710 (2020).
Weber, M. et al. Lower protein content in infant formula reduces BMI and obesity risk at school age: follow-up of a randomized trial. Am. J. Clin. Nutr. 99 , 1041–1051 (2014).
Cope, M. B. & Allison, D. B. Critical review of the World Health Organization’s (WHO) 2007 report on ‘evidence of the long‐term effects of breastfeeding: systematic reviews and meta‐analysis’ with respect to obesity. Obes. Rev. 9 , 594–605 (2008).
Totzauer, M. et al. Different protein intake in the first year and its effects on adiposity rebound and obesity throughout childhood: 11 years follow‐up of a randomized controlled trial. Pediatr. Obes. 17 , e12961 (2022).
Deren, K. et al. Consumption of sugar-sweetened beverages in paediatric age: a position paper of the European academy of paediatrics and the European Childhood Obesity Group. Ann. Nutr. Metab. 74 , 296–302 (2019).
Felső, R., Lohner, S., Hollódy, K., Erhardt, É. & Molnár, D. Relationship between sleep duration and childhood obesity: systematic review including the potential underlying mechanisms. Nutr. Metab. Cardiovasc. Dis. 27 , 751–761 (2017).
Farooq, A. et al. Longitudinal changes in moderate‐to‐vigorous‐intensity physical activity in children and adolescents: a systematic review and meta‐analysis. Obes. Rev. 21 , e12953 (2020).
Mahumud, R. A. et al. Association of dietary intake, physical activity, and sedentary behaviours with overweight and obesity among 282,213 adolescents in 89 low and middle income to high-income countries. Int. J. Obes. 45 , 2404–2418 (2021).
Ballon, M. et al. Socioeconomic inequalities in weight, height and body mass index from birth to 5 years. Int. J. Obes. 42 , 1671–1679 (2018).
Buoncristiano, M. et al. Socioeconomic inequalities in overweight and obesity among 6- to 9-year-old children in 24 countries from the World Health Organization European region. Obes. Rev. 22 , e13213 (2021).
Jiwani, S. S. et al. The shift of obesity burden by socioeconomic status between 1998 and 2017 in Latin America and the Caribbean: a cross-sectional series study. Lancet Glob. Health 7 , e1644–e1654 (2019).
Monteiro, C. A., Conde, W. L., Lu, B. & Popkin, B. M. Obesity and inequities in health in the developing world. Int. J. Obes. 28 , 1181–1186 (2004).
Guo, S. S. & Chumlea, W. C. Tracking of body mass index in children in relation to overweight in adulthood. Am. J. Clin. Nutr. 70 , 145S–148S (1999).
Aarestrup, J. et al. Birthweight, childhood overweight, height and growth and adult cancer risks: a review of studies using the Copenhagen School Health Records Register. Int. J. Obes. 44 , 1546–1560 (2020).
Eslam, M. et al. Defining paediatric metabolic (dysfunction)-associated fatty liver disease: an international expert consensus statement. Lancet Gastroenterol. Hepatol. 6 , 864–873 (2021).
Daniels, S. R. et al. Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation 111 , 1999–2012 (2005).
Cioana, M. et al. The prevalence of obesity among children with type 2 diabetes: a systematic review and meta-analysis. JAMA Netw. Open 5 , e2247186 (2022).
Gepstein, V. & Weiss, R. Obesity as the main risk factor for metabolic syndrome in children. Front. Endocrinol. 10 , 568 (2019).
Kuvat, N., Tanriverdi, H. & Armutcu, F. The relationship between obstructive sleep apnea syndrome and obesity: a new perspective on the pathogenesis in terms of organ crosstalk. Clin. Respir. J. 14 , 595–604 (2020).
Baker, J. L., Olsen, L. W. & Sorensen, T. I. Childhood body-mass index and the risk of coronary heart disease in adulthood. N. Engl. J. Med. 357 , 2329–2337 (2007).
Bjerregaard, L. G. et al. Change in overweight from childhood to early adulthood and risk of type 2 diabetes. N. Engl. J. Med. 378 , 1302–1312 (2018).
Kelsey, M. M., Zaepfel, A., Bjornstad, P. & Nadeau, K. J. Age-related consequences of childhood obesity. Gerontology 60 , 222–228 (2014).
Sharma, V. et al. A systematic review and meta-analysis estimating the population prevalence of comorbidities in children and adolescents aged 5 to 18 years. Obes. Rev. 20 , 1341–1349 (2019).
Lobstein, T. & Jackson-Leach, R. Planning for the worst: estimates of obesity and comorbidities in school-age children in 2025. Pediatr. Obes. 11 , 321–325 (2016).
Berthoud, H. R., Münzberg, H. & Morrison, C. D. Blaming the brain for obesity: integration of hedonic and homeostatic mechanisms. Gastroenterology 152 , 1728–1738 (2017).
Devoto, F. et al. Hungry brains: a meta-analytical review of brain activation imaging studies on food perception and appetite in obese individuals. Neurosci. Biobehav. Rev. 94 , 271–285 (2018).
Blum, W. F., Englaro, P., Attanasio, A. M., Kiess, W. & Rascher, W. Human and clinical perspectives on leptin. Proc. Nutr. Soc. 57 , 477–485 (1998).
Friedman, J. M. Leptin and the endocrine control of energy balance. Nat. Metab. 1 , 754–764 (2019).
Kühnen, P. et al. Proopiomelanocortin deficiency treated with a melanocortin-4 receptor agonist. N. Engl. J. Med. 375 , 240–246 (2016).
Clément, K. et al. Efficacy and safety of setmelanotide, an MC4R agonist, in individuals with severe obesity due to LEPR or POMC deficiency: single-arm, open-label, multicentre, phase 3 trials. Lancet Diabetes Endocrinol. 8 , 960–970 (2020).
Rosen, E. D. & Spiegelman, B. M. What we talk about when we talk about fat. Cell 156 , 20–44 (2014).
Fischer-Posovszky, P., Roos, J., Zoller, V. & Wabitsch, M. in Pediatric Obesity: Etiology, Pathogenesis and Treatment (ed. Freemark, M. S.) 81–93 (Springer, 2018).
Hammarstedt, A., Gogg, S., Hedjazifar, S., Nerstedt, A. & Smith, U. Impaired adipogenesis and dysfunctional adipose tissue in human hypertrophic obesity. Physiol. Rev. 98 , 1911–1941 (2018).
Silventoinen, K. et al. Genetic and environmental effects on body mass index from infancy to the onset of adulthood: an individual-based pooled analysis of 45 twin cohorts participating in the collaborative project of development of anthropometrical measures in twins (CODATwins) study. Am. J. Clin. Nutr. 104 , 371–379 (2016).
Silventoinen, K. et al. Differences in genetic and environmental variation in adult BMI by sex, age, time period, and region: an individual-based pooled analysis of 40 twin cohorts. Am. J. Clin. Nutr. 106 , 457–466 (2017).
Yengo, L. et al. Meta-analysis of genome-wide association studies for height and body mass index in approximately 700000 individuals of European ancestry. Hum. Mol. Genet. 27 , 3641–3649 (2018).
Vogelezang, S. et al. Novel loci for childhood body mass index and shared heritability with adult cardiometabolic traits. PLoS Genet. 16 , e1008718 (2020).
Bradfield, J. P. et al. A trans-ancestral meta-analysis of genome-wide association studies reveals loci associated with childhood obesity. Hum. Mol. Genet. 28 , 3327–3338 (2019). To our knowledge, currently the largest genome-wide association study meta-analysis on childhood obesity in >13,000 individuals with obesity and >15,500 controls.
Couto Alves, A. et al. GWAS on longitudinal growth traits reveals different genetic factors influencing infant, child, and adult BMI. Sci. Adv. 5 , eaaw3095 (2019).
Ding, X. et al. Genome-wide screen of DNA methylation identifies novel markers in childhood obesity. Gene 566 , 74–83 (2015).
Huang, R. C. et al. Genome-wide methylation analysis identifies differentially methylated CpG loci associated with severe obesity in childhood. Epigenetics 10 , 995–1005 (2015).
Rzehak, P. et al. DNA-methylation and body composition in preschool children: epigenome-wide-analysis in the European Childhood Obesity Project (CHOP)-Study. Sci. Rep. 7 , 14349 (2017).
Alfano, R. et al. Perspectives and challenges of epigenetic determinants of childhood obesity: a systematic review. Obes. Rev. 23 , e13389 (2022).
Vehmeijer, F. O. L. et al. DNA methylation and body mass index from birth to adolescence: meta-analyses of epigenome-wide association studies. Genome Med. 12 , 105 (2020). Meta-analysis of epigenome-wide association studies of childhood BMI in >4,000 children.
Richmond, R. C. et al. DNA methylation and BMI: investigating identified methylation sites at HIF3A in a causal framework. Diabetes 65 , 1231–1244 (2016).
Wahl, S. et al. Epigenome-wide association study of body mass index, and the adverse outcomes of adiposity. Nature 541 , 81–86 (2017).
Kivimäki, M. et al. Substantial intergenerational increases in body mass index are not explained by the fetal overnutrition hypothesis: the Cardiovascular Risk in Young Finns Study. Am. J. Clin. Nutr. 86 , 1509–1514 (2007).
Whitaker, R. C., Wright, J. A., Pepe, M. S., Seidel, K. D. & Dietz, W. H. Predicting obesity in young adulthood from childhood and parental obesity. N. Engl. J. Med. 337 , 869–873 (1997).
Davey Smith, G., Steer, C., Leary, S. & Ness, A. Is there an intrauterine influence on obesity? Evidence from parent child associations in the Avon Longitudinal Study of Parents and Children (ALSPAC). Arch. Dis. Child. 92 , 876–880 (2007).
Fleten, C. et al. Parent-offspring body mass index associations in the Norwegian Mother and Child Cohort Study: a family-based approach to studying the role of the intrauterine environment in childhood adiposity. Am. J. Epidemiol. 176 , 83–92 (2012).
Gaillard, R. et al. Childhood cardiometabolic outcomes of maternal obesity during pregnancy: the Generation R Study. Hypertension 63 , 683–691 (2014).
Lawlor, D. A. et al. Exploring the developmental overnutrition hypothesis using parental-offspring associations and FTO as an instrumental variable. PLoS Med. 5 , e33 (2008).
Patro, B. et al. Maternal and paternal body mass index and offspring obesity: a systematic review. Ann. Nutr. Metab. 63 , 32–41 (2013).
Sorensen, T. et al. Comparison of associations of maternal peri-pregnancy and paternal anthropometrics with child anthropometrics from birth through age 7 y assessed in the Danish National Birth Cohort. Am. J. Clin. Nutr. 104 , 389–396 (2016).
Styne, D. M. et al. Pediatric obesity – assessment, treatment, and prevention: an Endocrine Society Clinical Practice guideline. J. Clin. Endocrinol. Metab. 102 , 709–757 (2017).
National Institute for Health and Care Excellence. Obesity: identification, assessment and managenent: clinical guideline [CG189]. NICE https://www.nice.org.uk/guidance/cg189 (2022). A high quality clinical practice guideline for obesity management.
Barlow, S. E. Expert Committee Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 120 (Suppl. 4), S164–S192 (2007).
Canadian Task Force on Preventive Health Care. Recommendations for growth monitoring, and prevention and management of overweight and obesity in children and youth in primary care. Can. Med. Assoc. J. 187 , 411–421 (2015).
US Preventive Services Task Force. Screening for obesity in children and adolescents: US Preventive Services Task Force recommendation statement. JAMA 317 , 2417–2426 (2017).
McConnell-Nzunga, J. et al. Classification of obesity varies between body mass index and direct measures of body fat in boys and girls of Asian and European ancestry. Meas. Phys. Educ. Exerc. Sci. 22 , 154–166 (2018).
Reinehr, T. et al. Definable somatic disorders in overweight children and adolescents. J. Pediatr. 150 , 618–622.e5 (2007).
Reinehr, T. Thyroid function in the nutritionally obese child and adolescent. Curr. Opin. Pediatr. 23 , 415–420 (2011).
Kohlsdorf, K. et al. Early childhood BMI trajectories in monogenic obesity due to leptin, leptin receptor, and melanocortin 4 receptor deficiency. Int. J. Obes. 42 , 1602–1609 (2018).
Armstrong, S. et al. Physical examination findings among children and adolescents with obesity: an evidence-based review. Pediatrics 137 , e20151766 (2016).
Reinehr, T. & Roth, C. L. Is there a causal relationship between obesity and puberty? Lancet Child Adolesc. Health 3 , 44–54 (2019).
Garnett, S. P., Baur, L. A. & Cowell, C. T. Waist-to-height ratio: a simple option for determining excess central adiposity in young people. Int. J. Obes. 32 , 1028–1030 (2008).
Maffeis, C., Banzato, C., Talamini, G. & Obesity Study Group of the Italian Society of Pediatric Endocrinology and Diabetology. Waist-to-height ratio, a useful index to identify high metabolic risk in overweight children. J. Pediatr. 152 , 207–213.e2 (2008).
Hampl, S. E. et al. Clinical practice guideline for the evaluation and treatment of children and adolescents with obesity. Pediatrics 151 , e2022060640 (2023). A new, comprehensive clinical practice guideline outlining current recommendations on assessment and treatment of children and adolescents with obesity.
Reinehr, T. et al. Comparison of cardiovascular risk factors between children and adolescents with classes III and IV obesity: findings from the APV cohort. Int. J. Obes. 45 , 1061–1073 (2021).
Reinehr, T. Metabolic syndrome in children and adolescents: a critical approach considering the interaction between pubertal stage and insulin resistance. Curr. Diabetes Rep. 16 , 8 (2016).
Zeitler, P. et al. ISPAD Clinical Practice Consensus Guidelines 2018: type 2 diabetes mellitus in youth. Pediatr. Diabetes 19 , 28–46 (2018).
Ibáñez, L. et al. An International Consortium update: pathophysiology, diagnosis, and treatment of polycystic ovarian syndrome in adolescence. Horm. Res. Paediatr. 88 , 371–395 (2017).
Brockmann, P. E., Schaefer, C., Poets, A., Poets, C. F. & Urschitz, M. S. Diagnosis of obstructive sleep apnea in children: a systematic review. Sleep Med. Rev. 17 , 331–340 (2013).
Taylor, E. D. et al. Orthopedic complications of overweight in children and adolescents. Pediatrics 117 , 2167–2174 (2006).
Winck, A. D. et al. Effects of obesity on lung volume and capacity in children and adolescents: a systematic review. Rev. Paul. Pediatr. 34 , 510–517 (2016).
PubMed PubMed Central Google Scholar
Jebeile, H., Lister, N., Baur, L., Garnett, S. & Paxton, S. J. Eating disorder risk in adolescents with obesity. Obes. Rev. 22 , e13173 (2021).
Quek, Y. H., Tam, W. W. S., Zhang, M. W. B. & Ho, R. C. M. Exploring the association between childhood and adolescent obesity and depression: a meta-analysis. Obes. Rev. 18 , 742–754 (2017).
World Health Organization. Consideration of the Evidence on Childhood Obesity for the Commission on Ending Childhood Obesity . Report of the Ad Hoc Working Group on Science and Evidence for Ending Childhood Obesity (WHO, 2016).
Pickett, K. et al. The Child of the North: building a fairer future after COVID-19. The Northern Health Science Alliance and N8 Research Partnership https://www.thenhsa.co.uk/app/uploads/2022/01/Child-of-the-North-Report-FINAL-1.pdf (2021).
Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 32 , 513–531 (1977).
Nuffield Council on Bioethics. Public Health: Ethical Issues (Nuffield Council on Bioethics, 2007).
Lorenc, T., Petticrew, M., Welch, V. & Tugwell, P. What types of interventions generate inequalities? Evidence from systematic reviews. J. Epidemiol. Community Health 67 , 190–193 (2013).
Adams, J., Mytton, O., White, M. & Monsivais, P. Why are some population interventions for diet and obesity more equitable and effective than others? The role of individual agency. PLoS Med. 13 , e1001990 (2016).
Backholer, K. et al. A framework for evaluating the impact of obesity prevention strategies on socioeconomic inequalities in weight. Am. J. Public Health 104 , e43–e50 (2014).
McGill, R. et al. Are interventions to promote healthy eating equally effective for all? Systematic review of socioeconomic inequalities in impact. BMC Public Health 15 , 457 (2015).
Brown, T. et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 7 , Cd001871 (2019). A Cochrane review involving 153 RCTs of diet and/or physical activity interventions to prevent obesity in children and adolescents, highlighting varying effectiveness of interventions in different age groups.
PubMed Google Scholar
Le, L. K.-D. et al. Prevention of high body mass index and eating disorders: a systematic review and meta-analysis. Eat. Weight Disord. 27 , 2989–3003 (2022).
Nobles, J., Summerbell, C., Brown, T., Jago, R. & Moore, T. A secondary analysis of the childhood obesity prevention Cochrane Review through a wider determinants of health lens: implications for research funders, researchers, policymakers and practitioners. Int. J. Behav. Nutr. Phys. Act. 18 , 22 (2021).
Rai, K. K., Dogra, S. A., Barber, S., Adab, P. & Summerbell, C. A scoping review and systematic mapping of health promotion interventions associated with obesity in Islamic religious settings in the UK. Obes. Rev. 20 , 1231–1261 (2019).
World Health Organization. Nutrition Action in Schools: A Review of Evidence Related to the Nutrition-Friendly Schools Initiative (WHO, 2021).
Daly-Smith, A. et al. Using a multi-stakeholder experience-based design process to co-develop the Creating Active Schools Framework. Int. J. Behav. Nutr. Phys. Act. 17 , 13 (2020).
Tibbitts, B. et al. Considerations for individual-level versus whole-school physical activity interventions: stakeholder perspectives. Int. J. Environ. Res. Public Health https://doi.org/10.3390/ijerph18147628 (2021).
Askie, L. M. et al. Interventions commenced by early infancy to prevent childhood obesity-The EPOCH Collaboration: an individual participant data prospective meta-analysis of four randomized controlled trials. Pediatr. Obes. 15 , e12618 (2020). To our knowledge, the first prospective individual participant data meta-analysis showing that interventions commencing in late pregnancy or very early childhood are associated with healthier BMI z -score at age 18–24 months.
Seidler, A. L. et al. Examining the sustainability of effects of early childhood obesity prevention interventions: follow-up of the EPOCH individual participant data prospective meta-analysis. Pediatr. Obes. 17 , e12919 (2022).
Taylor, R. W. et al. Sleep, nutrition, and physical activity interventions to prevent obesity in infancy: follow-up of the prevention of overweight in infancy (POI) randomized controlled trial at ages 3.5 and 5 y. Am. J. Clin. Nutr. 108 , 228–236 (2018).
Mihrshahi, S. et al. A review of registered randomized controlled trials for the prevention of obesity in infancy. Int. J. Environ. Res. Public Health 18 , 2444 (2021).
Farooq, M. A. et al. Timing of the decline in physical activity in childhood and adolescence: Gateshead Millennium Cohort Study. Br. J. Sports Med. 52 , 1002–1006 (2018).
van Sluijs, E. M. F. et al. Physical activity behaviours in adolescence: current evidence and opportunities for intervention. Lancet 398 , 429–442 (2021).
Griffin, N. et al. A critique of the English national policy from a social determinants of health perspective using a realist and problem representation approach: the ‘Childhood Obesity: a plan for action’ (2016, 2018, 2019). BMC Public Health 21 , 2284 (2021).
Knai, C., Lobstein, T., Petticrew, M., Rutter, H. & Savona, N. England’s childhood obesity action plan II. Br. Med. J. 362 , k3098 (2018).
World Health Organization. WHO European Regional Obesity Report 2022 (WHO, 2022).
Zemrani, B., Gehri, M., Masserey, E., Knob, C. & Pellaton, R. A hidden side of the COVID-19 pandemic in children: the double burden of undernutrition and overnutrition. Int. J. Equity Health 20 , 44 (2021).
Alman, K. L. et al. Dietetic management of obesity and severe obesity in children and adolescents: a scoping review of guidelines. Obes. Rev. https://doi.org/10.1111/obr.13132 (2020).
Pfeiffle, S. et al. Current recommendations for nutritional management of overweight and obesity in children and adolescents: a structured framework. Nutrients https://doi.org/10.3390/nu11020362 (2019).
Scottish Intercollegiate Guidelines Network. Management of obesity. A National Clinical Guideline . SIGN 115 (SIGN, 2010).
Reinehr, T. et al. Two-year follow-up in 21,784 overweight children and adolescents with lifestyle intervention. Obesity 17 , 1196–1199 (2009).
Ells, L. J. et al. Interventions for treating children and adolescents with overweight and obesity: an overview of Cochrane reviews. Int. J. Obes. 42 , 1823–1833 (2018).
Al‐Khudairy, L. et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese adolescents aged 12 to 17 years. Cochrane Database Syst. Rev. 6 , CD012691 (2017). One of three Cochrane reviews looking at lifestyle treatment of paediatric obesity, in this case in adolescents, which identified 44 completed trials, finding low quality evidence of improvements in BMI and moderate quality evidence of improvements in weight.
Mead, E. et al. Diet, physical activity and behavioural interventions for the treatment of overweight or obese children from the age of 6 to 11 years. Cochrane Database Syst. Rev. 6 , CD012651 (2017). A Cochrane Review, involving 70 RCTs, showing that multicomponent behavioural interventions can lead to small, short-term reductions in BMI and related measures in children aged 6–11 years with obesity.
Ho, M. et al. Effectiveness of lifestyle interventions in child obesity: systematic review with meta-analysis. Pediatrics 130 , e1647–e1671 (2012). To our knowledge, the first systematic review of lifestyle interventions in children and adolescents with obesity to show improvements in cardiometabolic outcomes (LDL cholesterol, triglycerides, fasting insulin and blood pressure), as well as weight.
Clinical Practice Guideline Panel. Clinical practice guideline for multicomponent behavioral treatment of obesity and overweight in children and adolescents: current state of the evidence and research needs. American Psychological Association https://www.apa.org/obesity-guideline/clinical-practice-guideline.pdf (2018).
Nowicka, P. & Flodmark, C. E. Family therapy as a model for treating childhood obesity: useful tools for clinicians. Clin. Child. Psychol. Psychiatry 16 , 129–145 (2011).
Wilfley, D. E. et al. Improving access and systems of care for evidence-based childhood obesity treatment: conference key findings and next steps. Obesity 25 , 16–29 (2017).
Amiri, P. et al. Does motivational interviewing improve the weight management process in adolescents? A systematic review and meta-analysis. Int. J. Behav. Med. 29 , 78–103 (2022).
Kao, T. A., Ling, J., Hawn, R. & Vu, C. The effects of motivational interviewing on children’s body mass index and fat distributions: a systematic review and meta-analysis. Obes. Rev. 22 , e13308 (2021).
Hassapidou, M. et al. European Association for the Study of Obesity (EASO) position statement on medical nutrition therapy for the management of overweight and obesity in children and adolescents developed in collaboration with the European Federation of the Associations of Dietitians (EFAD). Obes. Facts https://doi.org/10.1159/000527540 (2022).
Hoelscher, D. M., Kirk, S., Ritchie, L. & Cunningham-Sabo, L. Position of the Academy of Nutrition and Dietetics: interventions for the prevention and treatment of pediatric overweight and obesity. J. Acad. Nutr. Diet. 113 , 1375–1394 (2013).
Hoare, J. K., Jebeile, H., Garnett, S. P. & Lister, N. B. Novel dietary interventions for adolescents with obesity: a narrative review. Pediatr. Obes. 16 , e12798 (2021).
Lister, N. et al. Nutritional adequacy of diets for adolescents with overweight and obesity: considerations for dietetic practice. Eur. J. Clin. Nutr. 71 , 646–651 (2017).
Andela, S. et al. Efficacy of very low-energy diet programs for weight loss: a systematic review with meta-analysis of intervention studies in children and adolescents with obesity. Obes. Rev. 20 , 871–882 (2019).
Srivastava, G. & Apovian, C. M. Current pharmacotherapy for obesity. Nat. Rev. Endocrinol. 14 , 12–24 (2018).
Apperley, L. J. et al. Childhood obesity: a review of current and future management options. Clin. Endocrinol. 96 , 288–301 (2022).
European Medicines Agency. Saxenda. European Medicines Agency https://www.ema.europa.eu/en/medicines/human/EPAR/saxenda (2022).
US Food and Drug Administration. FDA approves weight management drug for patients aged 12 and older. FDA https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-weight-management-drug-patients-aged-12-and-older (2021).
Kelly, A. S. et al. A randomized, controlled trial of liraglutide for adolescents with obesity. N. Engl. J. Med. 382 , 2117–2128 (2020). To our knowledge, the first RCT of liraglutide, administered daily via subcutaneous injection, in adolescents with obesity.
US Food and Drug Administration. FDA approves novel, dual-targeted treatment for type 2 iabetes. FDA https://www.fda.gov/news-events/press-announcements/fda-approves-novel-dual-targeted-treatment-type-2-diabetes (2022).
Jastreboff, A. M. et al. Tirzepatide once weekly for the treatment of obesity. N. Engl. J. Med. 387 , 205–216 (2022).
Holst, J. J. & Rosenkilde, M. M. GIP as a therapeutic target in diabetes and obesity: insight from incretin co-agonists. J. Clin. Endocrinol. Metab. https://doi.org/10.1210/clinem/dgaa327 (2020).
US National Library of Medicine. ClinicalTrials.gov https://clinicaltrials.gov/ct2/show/study/NCT05260021 (2023).
Müller, T. D., Blüher, M., Tschöp, M. H. & DiMarchi, R. D. Anti-obesity drug discovery: advances and challenges. Nat. Rev. Drug Discov. 21 , 201–223 (2022).
Chalklin, C. G., Ryan Harper, E. G. & Beamish, A. J. Metabolic and bariatric surgery in adolescents. Curr. Obes. Rep. 10 , 61–69 (2021).
Albaugh, V. L. et al. Regulation of body weight: lessons learned from bariatric surgery. Mol. Metab. https://doi.org/10.1016/j.molmet.2022.101517 (2022).
Uhe, I. et al. Roux-en-Y gastric bypass, sleeve gastrectomy, or one-anastomosis gastric bypass? A systematic review and meta-analysis of randomized-controlled trials. Obesity 30 , 614–627 (2022).
Inge, T. H. et al. Long-term outcomes of bariatric surgery in adolescents with severe obesity (FABS-5+): a prospective follow-up analysis. Lancet Diabetes Endocrinol. 5 , 165–173 (2017).
Olbers, T. et al. Laparoscopic Roux-en-Y gastric bypass in adolescents with severe obesity (AMOS): a prospective, 5-year, Swedish nationwide study. Lancet Diabetes Endocrinol. https://doi.org/10.1016/S2213-8587(16)30424-7 (2017).
Pratt, J. S. et al. ASMBS pediatric metabolic and bariatric surgery guidelines, 2018. Surg. Obes. Relat. Dis. 14 , 882–901 (2018).
Jarvholm, K. et al. 5-year mental health and eating pattern outcomes following bariatric surgery in adolescents: a prospective cohort study. Lancet Child Adolesc. Health 4 , 210–219 (2020).
Van Der Heijden, L., Feskens, E. & Janse, A. Maintenance interventions for overweight or obesity in children: a systematic review and meta‐analysis. Obes. Rev. 19 , 798–809 (2018).
Park, J., Park, M.-J. & Seo, Y.-G. Effectiveness of information and communication technology on obesity in childhood and adolescence: systematic review and meta-analysis. J. Med. Internet Res. 23 , e29003 (2021).
Brissman, M., Beamish, A. J., Olbers, T. & Marcus, C. Prevalence of insufficient weight loss 5 years after Roux-en-Y gastric bypass: metabolic consequences and prediction estimates: a prospective registry study. BMJ Open 11 , e046407 (2021).
El Ansari, W. & Elhag, W. Weight regain and insufficient weight loss after bariatric surgery: definitions, prevalence, mechanisms, predictors, prevention and management strategies, and knowledge gaps – a scoping review. Obes. Surg. 31 , 1755–1766 (2021).
World Health Organization Regional Office for Europe. Weight Bias and Obesity Stigma: Considerations for the WHO European Region (WHO, 2017).
Puhl, R. M. & Latner, J. D. Stigma, obesity, and the health of the nation’s children. Psychol. Bull. 133 , 557–580 (2007).
Black, W. R. et al. Health-related quality of life across recent pediatric obesity classification recommendations. Children 8 , 303 (2021).
Finne, E., Reinehr, T., Schaefer, A., Winkel, K. & Kolip, P. Changes in self-reported and parent-reported health-related quality of life in overweight children and adolescents participating in an outpatient training: findings from a 12-month follow-up study. Health Qual. Life Outcomes 11 , 1 (2013).
Hill, A. J. Obesity in children and the ‘myth of psychological maladjustment’: self-esteem in the spotlight. Curr. Obes. Rep. 6 , 63–70 (2017).
McGregor, S., McKenna, J., Gately, P. & Hill, A. J. Self‐esteem outcomes over a summer camp for obese youth. Pediatr. Obes. 11 , 500–505 (2016).
Jansen, P., Mensah, F., Clifford, S., Nicholson, J. & Wake, M. Bidirectional associations between overweight and health-related quality of life from 4–11 years: longitudinal study of Australian children. Int. J. Obes. 37 , 1307–1313 (2013).
Mannan, M., Mamun, A., Doi, S. & Clavarino, A. Is there a bi-directional relationship between depression and obesity among adult men and women? Systematic review and bias-adjusted meta analysis. Asian J. Psychiatr. 21 , 51–66 (2016).
Lindberg, L., Hagman, E., Danielsson, P., Marcus, C. & Persson, M. Anxiety and depression in children and adolescents with obesity: a nationwide study in Sweden. BMC Med. 18 , 30 (2020).
Jebeile, H. et al. Association of pediatric obesity treatment, including a dietary component, with change in depression and anxiety: a systematic review and meta-analysis. JAMA Pediatr. 173 , e192841 (2019).
Gow, M. L. et al. Pediatric obesity treatment, self‐esteem, and body image: a systematic review with meta‐analysis. Pediatr. Obes. 15 , e12600 (2020).
Jebeile, H. et al. Treatment of obesity, with a dietary component, and eating disorder risk in children and adolescents: a systematic review with meta-analysis. Obes. Rev. 20 , 1287–1298 (2019). To our knowledge, the first systematic review to show that structured and professionally led weight management interventions in children and adolescents with obesity are associated with reductions in eating disorder risk and symptoms.
Kjeldbjerg, M. L. & Clausen, L. Prevalence of binge-eating disorder among children and adolescents: a systematic review and meta-analysis. Eur. Child Adolesc. Psychiatry https://doi.org/10.1007/s00787-021-01850-2 (2021).
Patton, G. C., Selzer, R., Coffey, C., Carlin, J. B. & Wolfe, R. Onset of adolescent eating disorders: population based cohort study over 3 years. BMJ 318 , 765–768 (1999).
Cortese, S. The association between ADHD and obesity: intriguing, progressively more investigated, but still puzzling. Brain Sci. 9 , 256 (2019).
Griffiths, L. J., Dezateux, C. & Hill, A. Is obesity associated with emotional and behavioural problems in children? Findings from the Millennium Cohort Study. Int. J. Pediatr. Obes. 6 , e423–e432 (2011).
Harrist, A. W. et al. The social and emotional lives of overweight, obese, and severely obese children. Child. Dev. 87 , 1564–1580 (2016).
Van Geel, M., Vedder, P. & Tanilon, J. Are overweight and obese youths more often bullied by their peers? A meta-analysis on the relation between weight status and bullying. Int. J. Obes. 38 , 1263–1267 (2014).
Albuquerque, D., Nóbrega, C., Manco, L. & Padez, C. The contribution of genetics and environment to obesity. Br. Med. Bull. 123 , 159–173 (2017).
Rancourt, D. & McCullough, M. B. Overlap in eating disorders and obesity in adolescence. Curr. Diabetes Rep. 15 , 78 (2015).
House, E. T. et al. Identifying eating disorders in adolescents and adults with overweight or obesity: a systematic review of screening questionnaires. Int. J. Eat. Disord. 55 , 1171–1193 (2022).
Lister, N. B., Baur, L. A., Paxton, S. J. & Jebeile, H. Contextualising eating disorder concerns for paediatric obesity treatment. Curr. Obes. Rep. 10 , 322–331 (2021).
Hagman, E. et al. Effect of an interactive mobile health support system and daily weight measurements for pediatric obesity treatment, a 1-year pragmatical clinical trial. Int. J. Obes. 46 , 1527–1533 (2022).
Swinburn, B. A. et al. The global syndemic of obesity, undernutrition, and climate change: The Lancet commission report. Lancet 393 , 791–846 (2019).
Whitehead, M., Taylor-Robinson, D. & Barr, B. Poverty, health, and covid-19. Br. Med. J. 372 , n376 (2021).
Morrison, K. M. et al. The CANadian Pediatric Weight Management Registry (CANPWR): lessons learned from developing and initiating a national, multi-centre study embedded in pediatric clinical practice. BMC Pediatr. 18 , 237 (2018).
Kirk, S. et al. Establishment of the pediatric obesity weight evaluation registry: a national research collaborative for identifying the optimal assessment and treatment of pediatric obesity. Child. Obes. 13 , 9–17 (2017).
Hagman, E., Danielsson, P., Lindberg, L. & Marcus, C., BORIS Steering Committee. Paediatric obesity treatment during 14 years in Sweden: lessons from the Swedish Childhood Obesity Treatment Register – BORIS. Pediatr. Obes. 15 , e12626 (2020).
Bohn, B. et al. Changing characteristics of obese children and adolescents entering pediatric lifestyle intervention programs in Germany over the last 11 years: an adiposity patients registry multicenter analysis of 65,453 children and adolescents. Obes. Facts 10 , 517–530 (2017).
Seidler, A. L. et al. A guide to prospective meta-analysis. BMJ 367 , l5342 (2019).
Hunter, K. E. et al. Transforming obesity prevention for children (TOPCHILD) collaboration: protocol for a systematic review with individual participant data meta-analysis of behavioural interventions for the prevention of early childhood obesity. BMJ Open 12 , e048166 (2022).
Lister, N. B. et al. Eating disorders in weight-related therapy (EDIT) collaboration: rationale and study design. Nutr. Res. Rev. https://doi.org/10.1017/S0954422423000045 (2023).
Hadjiyannakis, S. et al. Obesity class versus the Edmonton Obesity Staging System for Pediatrics to define health risk in childhood obesity: results from the CANPWR cross-sectional study. Lancet Child Adolesc. Health 3 , 398–407 (2019).
Brown, V. et al. Core outcome set for early intervention trials to prevent obesity in childhood (COS-EPOCH): agreement on “what” to measure. Int. J. Obes. 46 , 1867–1874 (2022). A stakeholder-informed study that identified the minimum outcomes recommended for collecting and reporting in obesity prevention trials in early childhood.
Han, J. C., Lawlor, D. A. & Kimm, S. Y. Childhood obesity. Lancet 375 , 1737–1748 (2010).
Shin, A. C., Zheng, H. & Berthoud, H. R. An expanded view of energy homeostasis: neural integration of metabolic, cognitive, and emotional drives to eat. Physiol. Behav. 97 , 572–580 (2009).
Lennerz, B., Wabitsch, M. & Eser, K. Ätiologie und genese [German]. Berufl. Rehabil. 1 , 14 (2014).
Google Scholar
Pont, S. J., Puhl, R., Cook, S. R. & Slusser, W. Stigma experienced by children and adolescents with obesity. Pediatrics 140 , e20173034 (2017).
Talumaa, B., Brown, A., Batterham, R. L. & Kalea, A. Z. Effective strategies in ending weight stigma in healthcare. Obes. Rev. 23 , e13494 (2022).
Rubino, F. et al. Joint international consensus statement for ending stigma of obesity. Nat. Med. 26 , 485–497 (2020).
Download references
Author information
Authors and affiliations.
Children’s Hospital Westmead Clinical School, Sydney Medical School, The University of Sydney, Sydney, New South Wales, Australia
Natalie B. Lister & Louise A. Baur
Institute of Endocrinology and Diabetes, The Children’s Hospital at Westmead, Sydney, New South Wales, Australia
Natalie B. Lister
Sydney School of Public Health, The University of Sydney, Sydney, New South Wales, Australia
Louise A. Baur
Weight Management Services, The Children’s Hospital at Westmead, Sydney, New South Wales, Australia
The Generation R Study Group, Erasmus MC, University Medical Center Rotterdam, Rotterdam, Netherlands
Janine F. Felix
Department of Paediatrics, Erasmus MC, University Medical Center Rotterdam, Rotterdam, Netherlands
Institute of Health Sciences, School of Medicine, University of Leeds, Leeds, UK
Andrew J. Hill
Division of Paediatrics, Department of Clinical Science Intervention and Technology, Karolinska Institutet and Karolinska University Hospital, Stockholm, Sweden
Claude Marcus
Vestische Hospital for Children and Adolescents Datteln, University of Witten/Herdecke, Datteln, Germany
Thomas Reinehr
Department of Sport and Exercise Sciences, Durham University, Durham, UK
- Carolyn Summerbell
Division of Paediatric Endocrinology and Diabetes, Department of Paediatrics and Adolescent Medicine, Ulm University Medical Centre, Ulm, Germany
Martin Wabitsch
You can also search for this author in PubMed Google Scholar
Contributions
Introduction (L.A.B., J.F.F. and N.B.L.); Epidemiology (L.A.B. and J.F.F.); Mechanisms/pathophysiology (L.A.B., J.F.F., T.R. and M.W.); Diagnosis, screening and prevention (L.A.B., N.B.L., T.R., C.S. and M.W.); Management (L.A.B., N.B.L., A.J.H., C.M. and T.R.); Quality of life (L.A.B., N.B.L. and A.J.H.); Outlook (L.A.B., N.B.L., J.F.F., A.J.H., C.M., T.R., C.S. and M.W.); Overview of the Primer (L.A.B. and N.B.L.).
Corresponding author
Correspondence to Louise A. Baur .
Ethics declarations
Competing interests.
A.J.H. reports receiving payment for consultancy advice for Slimming World (UK). L.A.B. reports receiving honoraria for speaking in forums organized by Novo Nordisk in relation to management of adolescent obesity and the ACTION-Teens study, which is sponsored by Novo Nordisk. L.A.B. is the Australian lead of the study. T.R. received funding from the German Federal Ministry of Education and Research (BMBF; 01GI1120A/B) as part of the German Competence Network Obesity (Consortium ‘Youth with Extreme Obesity’). T.R. receives payment for consultancy advice related to pharmacological treatment of obesity from Novo Nordisk and Lilly, as well as honoraria for lectures in symposia organized by Novo Nordisk, Novartis and Merck. C.M. receives payments for consultancy advice and advisory board participation from Novo Nordisk, Oriflame Wellness, DeFaire AB and Itrim AB. C.M. also receives honoraria for speaking at meetings organized by Novo Nordisk and Astra Zeneca. C.M. is a shareholder and founder of Evira AB, a company that develops and sells systems for digital support for weight loss, and receives grants from Novo Nordisk for epidemiological studies of the effects of weight loss on future heath. M.W. received funding from the German Federal Ministry of Education and Research (BMBF; 01GI1120A/B) as part of the German Competence Network Obesity (Consortium ‘Youth with Extreme Obesity’). M.W. receives payment for consultancy advice related to pharmacological treatment of obesity from Novo Nordisk, Regeneron, Boehringer Ingelheim and LG Chem, as well as honoraria for speaking in symposia organized by Novo Nordisk, Rhythm Pharmaceuticals and Infectopharm. M.W. is principal investigator in phase II and phase III studies of setmelanotide sponsored by Rhythm Pharmaceuticals. N.B.L., J.F.F. and C.S. declare no competing interests.
Peer review
Peer review information.
Nature Reviews Disease Primers thanks C. Maffeis, L. Moreno, R, Weiss and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Cite this article.
Lister, N.B., Baur, L.A., Felix, J.F. et al. Child and adolescent obesity. Nat Rev Dis Primers 9 , 24 (2023). https://doi.org/10.1038/s41572-023-00435-4
Download citation
Accepted : 12 April 2023
Published : 18 May 2023
DOI : https://doi.org/10.1038/s41572-023-00435-4
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
This article is cited by
Relationship between 24-h activity behavior and body fat percentage in preschool children: based on compositional data and isotemporal substitution analysis.
BMC Public Health (2024)
Young people's experiences of physical activity insecurity: a qualitative study highlighting intersectional disadvantage in the UK
- Caroline Dodd-Reynolds
- Naomi Griffin
Enough with simplifying: “eat less and move more”: at what point are we with the treatment of excess weight in paediatrics?
- Giovanni Corsello
- Sergio Bernasconi
Italian Journal of Pediatrics (2024)
Association between watching eating broadcast “Mukbang and Cookbang” and body mass index status in South Korean adolescents stratified by gender
- Sang-yeon Park
- Jeongha Eom
- Eun-Cheol Park
Nutrition Journal (2024)
Effect of a carbohydrate-restricted diet on weight loss in overweight and obese pediatric population: a meta-analysis of randomized controlled trials
- Pejman Rohani
- Zahra Rasoulizadeh
- Nathalia Sernizon Guimarães
Diabetology & Metabolic Syndrome (2024)
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

- Search Menu
- Sign in through your institution
- Advance articles
- Special Issues
- Author Guidelines
- Submission Site
- Open Access
- Self Archiving Policy
- Why publish with this journal?
- About Translational Behavioral Medicine
- About Society of Behavioral Medicine
- Journal Staff
- Advertising and Corporate Services
- Journals Career Network
- Journals on Oxford Academic
- Books on Oxford Academic

Article Contents
Introduction, nih efforts, gaps and opportunities, acknowledgments, compliance with ethical standards.
- < Previous
Childhood obesity research at the NIH: Efforts, gaps, and opportunities
- Article contents
- Figures & tables
- Supplementary Data
S Sonia Arteaga, Layla Esposito, Stavroula K Osganian, Charlotte A Pratt, Jill Reedy, Deborah Young-Hyman, Childhood obesity research at the NIH: Efforts, gaps, and opportunities, Translational Behavioral Medicine , Volume 8, Issue 6, December 2018, Pages 962–967, https://doi.org/10.1093/tbm/iby090
- Permissions Icon Permissions
Childhood obesity is a major public health challenge. This article describes an overview of the National Institutes of Health (NIH) behavioral and social sciences childhood obesity research efforts. The overview will highlight five areas of childhood obesity research supported by the NIH: (a) basic behavioral and social sciences; (b) early childhood; (c) policies, programs, and environmental strategies; (d) health disparities; and (e) transagency and public–private collaboration. The article also describes potential gaps and opportunities in the areas of childhood obesity and severe obesity, measurement, and sleep.
Practice: The National Institutes of Health (NIH) supports a number of funding announcements, workshops, and dietary assessment tools related to childhood obesity.
Policy: Childhood obesity continues to be a major public health challenge, and research related to programs, policies, and/or environmental strategies could be further explored to assess factors related to the promotion of healthy weight among children.
Research: To address the childhood obesity epidemic, the NIH supports a broad spectrum of biomedical and behavioral research that seeks to identify the causes and consequences of childhood obesity to develop new and more effective approaches to its prevention and treatment, and synergize and disseminate evidence within the NIH and with other stakeholder organizations.
Childhood obesity continues to be a major public health challenge with 18.5% of children aged 2–19 years having obesity [ 1 ]. Despite earlier reports that there may be stabilization of obesity among children [ 2 ], recent findings suggest that obesity is not decreasing and severe obesity is increasing among Hispanic children [ 3 , 4 ]. Children who have obesity are more likely to have cardiovascular risk factors [ 5 , 6 ], type 2 diabetes [ 7 ], and are at increased risk for morbidity and mortality as adults [ 8 ] including increased risk of developing several types of cancer [ 9 ].
To address the childhood obesity epidemic, the National Institutes of Health (NIH) supports a broad spectrum of biomedical and behavioral research that seeks to identify the causes and consequences of childhood obesity and to develop new and more effective approaches to its prevention and treatment [ 10 ]. The childhood obesity research that NIH supports includes studies in pregnancy, infancy, childhood, adolescence, and prevention and treatment approaches in families, schools, and other community settings, as well as in health care settings. The NIH also supports basic behavioral and social science research that is providing insights into factors related to the development, prevention, and treatment of childhood obesity, as well as environmental and policy-related research.
In the following section, we provide an overview of the NIH behavioral and social sciences childhood obesity research efforts. This overview is not meant to be a comprehensive summary of NIH’s childhood obesity activities, but instead is based on active and recently completed NIH-funded research activities including workshops and funding announcements as they relate to the behavioral and social sciences. This overview highlights five areas of childhood obesity research supported by the NIH: (a) basic behavioral and social sciences; (b) early childhood; (c) policies, programs, and environmental strategies; (d) health disparities; and (e) transagency and public–private collaboration. Based on research findings and workshop recommendations, discussions on potential gaps and future opportunities in childhood obesity research are provided.
Basic behavioral and social sciences research in childhood obesity
The NIH has long recognized the importance of basic behavioral and social science research related to pediatric obesity and has supported numerous efforts through various Institute and Center initiatives as well as through investigator-initiated research [ 11 ]. In particular, one major initiative, the Obesity-Related Behavioral Intervention Trials (ORBIT) consortium ( www.nihorbit.org ), was a trans-NIH program led by the National Heart, Lung, and Blood Institute (NHLBI) that facilitated the translation of basic behavioral and social science findings into pediatric and adult obesity-related interventions [ 12 ]. The findings from ORBIT and other investigator-initiated research have advanced our understanding of several drivers of food intake and eating behaviors such as taste preferences, self-regulation, impulsivity, sensitization to the relative reinforcing value of food, food reward and inhibition, emotional eating, habituation to food, and ability to delay gratification [ 13 ]. Another important trans-NIH initiative is the Science of Behavior Change (SOBC) that focuses on understanding mechanisms for novel targets of behavior change. Self-regulation, stress resilience and reactivity, and interpersonal and social processes have all been identified by SOBC as promising targets of behavior change and intervention development [ 14 ], and all of these targets can be considered relevant for obesity prevention and control.
Despite significant advances in our understanding of eating behaviors, the individual characteristics and processes that predict and explain physical activity behaviors are not well understood. In response, the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) held a Workshop on Behavioral Phenotyping of Physical Activity and Sedentary Behavior in December 2015 to identify gaps and promising research opportunities in behavioral and psychological phenotyping related to variation in physical activity and sedentary behaviors as they relate to obesity [ 15 ]. This workshop resulted in the release of an NIDDK-led, trans-NIH program announcement (PAR-18–105) Ancillary Studies to Identify Behavioral and/or Psychological Phenotypes Contributing to Obesity.
Finally, research has demonstrated that characterizing and influencing individuals’ behaviors in relation to obesity prevention and treatment is increasingly complex and will require more personalized intervention approaches. Individuals’ behaviors do not operate in a vacuum nor are individuals necessarily characterized by one behavioral phenotype[ 16 ]. Future research in this area could work toward deciphering underlying behavioral mechanisms and developing theoretical frameworks that incorporate a more comprehensive and interdisciplinary approach, identifying patterns of behavioral and psychosocial phenotypes in the context of their various environmental influences.
Early childhood
Early childhood is a critical time period in the development of obesity, and the NIH supports several efforts focusing on the prenatal period through age 5. Recognizing the importance of the role of early childhood in the development of obesity, the NIH sponsored a 2013 workshop on the “Prevention of Obesity in Infancy and Early Childhood” [ 17 ], which resulted in a funding announcement, PA-18–032: Understanding Factors in Infancy and Early Childhood (Birth to 24 Months) that Influence Obesity Development (R01 Clinical Trial Optional).
In addition to studying obesity during infancy, the NIH also recognizes the importance of trans-generational impacts and has two large research initiatives that offer opportunities to better explore the trans-generational effects of obesity and its mechanisms: (a) Lifestyle Interventions for Expectant Moms (LIFE-Moms) and (b) Environmental influences on Child Health Outcomes (ECHO) program. Pregnancy is an opportunity to intervene and influence outcomes for the mother and offspring. In 2011, the NIH launched the LIFE-Moms consortium to determine whether behavioral and lifestyle interventions in overweight and obese pregnancy would have an effect on excessive gestational weight gain and impact maternal and child outcomes [ 18 ]. The findings from the LIFE-Moms consortium show that women randomized to the intervention group gained less weight compared with the standard care group [ 19 ]. The de-identified LIFE-Moms data will be available for investigators to access and analyze for future manuscripts. For more information, see https://repository.niddk.nih.gov/home/ .
In 2016, the NIH launched ECHO to fund multiple, synergistic, longitudinal studies using 83 pediatric cohorts to investigate environmental exposures—including physical, chemical, biological, social, behavioral, natural, and built environments—on child health and development [ 20 ]. Obesity is a key pediatric outcome with data to be contributed by all cohorts, enabling investigators to explore how obesity emerges from a complex web of exposures in early childhood. Future research could continue to explore the mechanisms of how early-life exposures contribute to the development of obesity and what factors (e.g., home and pediatric settings) may be leveraged to encourage healthy weight development.
Policies, programs, and environmental strategies
Policies, programs, and environmental strategies have an important influence on childhood obesity, but how and to what extent they affect childhood obesity warrants further study. Many of the factors addressable by policy and environmental change, such as large infrastructure changes or implementation of taxes or subsidies, are not under the control of researchers and may not be studied using traditional randomized study designs, relying instead on a study design referred to as a natural experiment [ 21 ]. A 2010 Institute of Medicine report and 2011 NIH Strategic Plan for Obesity recommended increased emphasis on evaluation of policy and environmental changes to determine their impact on improved diet, physical activity, and weight outcomes [ 22 , 23 ].
The NIH supports the evaluation of natural experiments through funding announcements PAR-17–178: Evaluating Natural Experiments in Healthcare to Improve Diabetes Prevention and Treatment (R18), PA-16–165: Obesity Policy Evaluation Research (R01), and PAR-18-854: Time-Sensitive Obesity Policy and Program Evaluation (R01). The grants funded through the aforementioned funding announcements cover a wide range of policy and environmental strategies including changes to the built environment through light rails, parks, and transportation improvements and the influence on physical activity and health; policies targeting sugar-sweetened beverages and the impact on diet and added sugars; and how later school start times are associated with weight and health outcomes among adolescents.
In addition to investigator-initiated research, the NIH has also launched large initiatives to assess how multi-level environmental factors affect childhood obesity. The NIH Healthy Communities Study was an observational study of 130 diverse communities that sought to determine the associations between characteristics of community programs and policies and body mass index (BMI), diet, and physical activity in children [ 24 ]. Data were collected on children (retrospectively up to 10 years using medical abstraction), their parents, the home environment, school lunch and physical activity environments, and community programs and policies (retrospectively up to 10 years). The results show that over time, more intense programs and policies are related to lower childhood BMI and that there are disparities in this association by sociodemographic family and community characteristics [ 25 ]. A de-identified public use dataset of the Healthy Communities Study is available for researchers to access at https://biolincc.nhlbi.nih.gov/home/ . Future research could investigate how contextual factors within communities (e.g., race/ethnicity of the community, crime, housing) interact with community programs and policies to promote healthy or obesogenic environments.
Health disparities
Obesity prevalence has risen to epidemic levels, particularly among various racial and ethnic minority groups, including Hispanics, African Americans, American Indians/Alaskan Natives, and low-income populations both in urban and rural communities and in all age groups across the lifespan [ 2 ]. To promote the health of future generations of adults, many NIH institutes have funded research addressing health disparities to gain a better understanding of the etiology of obesity as well as interventions that would lower the prevalence of obesity. The Childhood Obesity Prevention and Treatment Research (COPTR) consortium is an example of a large NIH initiative addressing health disparities and childhood obesity. COPTR tested multi-level multicomponent intervention approaches [ 26 ] to prevent excess weight gain in nonoverweight and overweight youth and to reduce weight in obese and severely obese youth [ 27 ]. Research funded under this consortium targeted preschoolers (2–5 years old) and preadolescents and adolescents (7–15 years old) with a total sample size of ~1,750 ( N ~50% females and ~70% minorities) for 3 years of intervention [ 27 ]. Two obesity prevention trials tested approaches that target home, community, and primary care settings for preschool children living in low-income and ethnically diverse neighborhoods. Two obesity treatment trials examined therapies for overweight and obese children, 7–15 years old, in school and home settings in collaboration with local youth organizations. The findings from COPTR could contribute to future understanding of the multiple factors, including social determinants of health indicators, to prevent or treat obesity among a diverse population of low-income children [ 28 , 29 ].
Recently, NIH staff led a systematic review of interventions addressing obesity disparities with the goal of providing guidance for future research, particularly in populations with a high prevalence of obesity and obesity-related cardiometabolic risk. The review noted a dearth of high-quality research that targets minority populations and a limited number of clinical trials in youth [ 30 ]. NIH staff also convened workshops such as the Multi-Level Intervention Research Methods: Recommendations for Targeting Hard-to-Reach, High-Risk or Vulnerable Populations and Communities. Recommendations from the workshop have been published elsewhere [ 31 ] and include recommendations under the following topics: study design and analytical approaches, intervention implementation, cultural adaptation of intervention, use of community health workers, and training of interventionists. Funding opportunity announcements that are relevant to health disparities research include PA-18–412: Addressing Health Disparities in NIDDK Diseases (R01 Clinical Trial Not Allowed); PA-18–152: Reducing Health Disparities Among Minority and Underserved Children (R01 Clinical Trial Optional); and PA-18–169: Reducing Health Disparities Among Minority and Underserved Children (R21 Clinical Trial Optional). Future research needs to better understand the biological and behavioral mechanisms of childhood obesity as well as the contextual and environmental factors that may alleviate or exacerbate obesity disparities [ 32 ].
Transagency and public–private partnership
Launched in 2009, the National Collaborative on Childhood Obesity Research (NCCOR; www.nccor.org ) brings together the nation’s four largest childhood obesity research funders—Centers for Disease Control and Prevention, NIH, United States Department of Agriculture, and Robert Wood Johnson Foundation—in a public–private collaboration to accelerate progress in reducing childhood obesity. Major NCCOR foci are identifying and evaluating practical and sustainable interventions; improving research resources (see Measurement section in this article for examples) to facilitate childhood obesity research and program evaluation; providing national leadership to accelerate implementation of evidence-informed practice and policy; and developing synergistic childhood obesity initiatives across multiple stakeholders [ 33 ].
NCCOR uses this collaborative approach to combine resources and expertise from stakeholder organizations to identify emerging areas of research need, formulate projects within the scope of the NCCOR mission, and identify external collaborators and funding sources by which to implement projects. Examples of NCCOR NIH led or co-led activities include (a) the Healthy Communities Study ( https://www.nhlbi.nih.gov/science/healthy-communities-study-hcs/ ), (b) the Johns Hopkins Global Obesity Center ( www.globalobesity.org ), (c) the Envision Research Network ( https://www.nccor.org/envision/publications.html ), and (d) the Childhood Obesity Declines ( https://www.nccor.org/projects/obesity-declines/ ) among others. Of note is that NCCOR recognizes that many and varied research design and evaluation approaches are needed to better understand the difficulties in reducing rates of childhood obesity, especially in the context of community-based initiatives. Thus, the initiatives cited here span research efforts, targeting individual behavior change to policy implementation, environmental to systemic social determinants of childhood obesity, and recognize the importance of community and academic partnerships. In addition to facilitating research resources and improving intervention and research methods, NCCOR is dedicated to the dissemination of promising evidence regarding intervention strategies and evidence-informed programs to policy makers and program implementers, particularly those embedded in the community and those addressing health inequities and underserved communities. Future research could continue to explore how partnerships with various entities such as housing, transportation, education, and social services can work together to more effectively deliver childhood obesity interventions.
In addition to the abovementioned NIH efforts, severe obesity, measurement issues in childhood obesity research, and the mechanisms associated with sleep and obesity have emerged as gaps and opportunities for further childhood obesity research.
Severe obesity
Severe obesity in youth, defined as BMI ≥ 1.2 times the 95th percentile or an absolute BMI ≥ 35 kg/m 2 , is a prevalent and serious disease with a limited number of effective and safe treatment options [ 34 ]. The prevalence of severe obesity among all children is 5.6% and is highest (7.7%) among adolescents aged 12–19 years [ 3 ]. To address the issue of severe obesity among adolescents, a workshop led by NIDDK, in cooperation with several NIH Institutes and Centers, entitled “Developing Precision Medicine Approaches to the Treatment of Severe Obesity in Adolescents” ( https://www.niddk.nih.gov/news/meetings-workshops/2017/workshop-developing-precision-medicine-approaches-treatment-severe-obesity-adolescents ) was convened in September 2017 to explore the current state of the science and identify (a) what is known regarding the epidemiology and biopsychosocial determinants of severe obesity in adolescents, (b) what is known regarding effectiveness of treatments for severe obesity in adolescents and predictors of response, and (c) gaps and opportunities for future research to develop more effective and targeted treatments for adolescents with severe obesity. Several gaps were identified and recommendations were made for opportunities to accelerate research to advance precision medicine approaches to treat severe obesity in adolescents and to enhance methodological rigor in pediatric obesity research. More research is needed to better understand the underlying etiology and pathophysiology of severe obesity in children and developing effective intervention approaches.
Measurement
Measurement is a fundamental component of all forms of research, including research on childhood obesity. The development and consistent use of high-quality, comparable measures and research methods is a priority. To address this need and encourage innovative research with novel assessment approaches, better statistical methods and modeling, and tools for culturally diverse populations and/or children at various ages, the NIH supports the Diet and Physical Activity Assessment Methodology (PA-16–167). However, the advancement and application of appropriate diet and physical activity measures remains challenging, as highlighted at two workshops at NIH, “Extending Dietary Patterns Research Methods” [ 35 ] and “Research Strategies for Nutritional and Physical Activity Epidemiology and Cancer Prevention” [ 36 ].
NIH resources are available to provide guidance on selecting measures and to provide tools for research. For example, NCI developed the Dietary Assessment Primer ( https://dietassessmentprimer.cancer.gov/ ) to help determine the best way to assess diet, and specific dietary assessment tools, such as the Automated Self-Administered 24-Hour (ASA24; https://epi.grants.cancer.gov/asa24/ ) and Dietary Assessment Tool and the Diet History Questionnaire ( https://epi.grants.cancer.gov/dhq2/ ). In addition, NCCOR’s Measures Registry and User Guides ( https://www.nccor.org/nccor-tools/measures/ ) were developed for four relevant domains, including diet, physical activity, food environment, and physical activity environment, and were designed to provide an overview of measurement, describe general principles of measurement selection, present case studies, and direct researchers to additional resources across the lifespan.
Although these tools are useful, opportunities exist to further develop objective measurements of diet and physical activity through new technologies that integrate and exploit advances in wearable sensors and other novel image-based tools. More sophisticated exposure characterization for childhood obesity researchers could allow for measurement of individual diet and physical activity behaviors as well as a linkage in real time to other details that include geospatial location, time, and context, providing opportunities to examine new research questions and identify potential targets for intervention.
Sleep and obesity
Recent meta-analyses have found an association between shortened sleep duration and increased risk of obesity in children [ 37–39 ]. The relationship between sleep and obesity is stronger in younger children than in adolescents [ 37 ], and more research is needed to better understand why the relationship varies with age. Future research could also investigate the mechanisms of sleep/circadian rhythms and the development of obesity including how in utero factors may affect those mechanisms. Sleep is a modifiable behavior, and research is needed to better understand how improving sleep may affect weight gain, weight loss, and weight maintenance. For instance, a recent study found that it was possible to increase sleep in children, and the increased sleep condition versus decreased sleep condition was associated with lower self-reported caloric intake and weight, but the study was short in duration and had a small sample size [ 40 ]. More research is needed to better understand how intervention approaches including sleep can lead to the prevention and treatment of obesity. Furthermore, future research could address how health disparities may interact with sleep to affect obesity. NIH is currently supporting funding announcement PAR-17–234: Mechanisms and Consequences of Sleep Disparities in the U.S. (R01).
This article highlights NIH childhood obesity research efforts in the behavioral and social sciences. There are several activities that the NIH has undertaken to further the knowledge, prevention, and treatment of childhood obesity. In addition to the aforementioned NIH efforts, there are emerging gaps and opportunities related to severe obesity, measurement issues, and sleep and obesity. The childhood obesity epidemic continues to grow, and the NIH is committed to supporting research that will help alleviate the obesity epidemic. NIH will continue to support behavioral and social science approaches to better understand the drivers of childhood obesity and to develop effective interventions.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute, Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institute of Diabetes and Digestive and Kidney Diseases, National Cancer Institute, Office of Behavioral and Social Science Research, the National Institutes of Health, or the U.S. Department of Health and Human Services.
Funding: This commentary was not funded.
Conflicts of Interest: All authors declare they have no conflicts of interest.
Ethical Approval: Human rights, informed consent, and animal welfare ethical statements are not applicable.
Hales CM , Carroll MD , Fryar CD , Ogden CL . Prevalence of obesity among adults and youth: United States, 2015–2016 . NCHS Data Brief . 2017 October;( 288 ): 1 – 8 .
Google Scholar
Ogden CL , Carroll MD , Lawman HG , et al. Trends in obesity prevalence among children and adolescents in the United States, 1988–1994 through 2013–2014 . JAMA . 2016 ; 315 ( 21 ): 2292 – 2299 .
Hales CM , Fryar CD , Carroll MD , Freedman DS , Ogden CL . Trends in obesity and severe obesity prevalence in us youth and adults by sex and age, 2007–2008 to 2015–2016 . JAMA . 2018;319(16):1723–1725 . doi: 10.1001/jama.2018.3060
Skinner AC , Ravanbakht SN , Skelton JA , Perrin EM , Armstrong SC . Prevalence of obesity and severe obesity in US children, 1999–2016 . Pediatrics . 2018;141(3):e20173459 . doi: 10.1542/peds.2017–3459
Freedman DS , Mei Z , Srinivasan SR , Berenson GS , Dietz WH . Cardiovascular risk factors and excess adiposity among overweight children and adolescents: the Bogalusa Heart Study . J Pediatr . 2007 ; 150 ( 1 ): 12 – 17.e2 .
Koskinen J , Juonala M , Dwyer T , et al. Impact of lipid measurements in youth in addition to conventional clinic-based risk factors on predicting preclinical atherosclerosis in adulthood: International Childhood Cardiovascular Cohort Consortium . Circulation . 2018 ; 137 ( 12 ): 1246 – 1255 .
Goran MI , Ball GD , Cruz ML . Obesity and risk of type 2 diabetes and cardiovascular disease in children and adolescents . J Clin Endocrinol Metab . 2003 ; 88 ( 4 ): 1417 – 1427 .
Reilly JJ , Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review . Int J Obes (Lond) . 2011 ; 35 : 891 – 898 .
World Cancer Research Fund/American Institute for Cancer Research . Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective . Washington, DC: American Institute for Cancer Research ; 2007 .
Google Preview
Rodgers GP , Collins FS . The next generation of obesity research: no time to waste . JAMA . 2012 ; 308 ( 11 ): 1095 – 1096 .
Czajkowski SM . National Institutes of Health update: translating basic behavioral science into new pediatric obesity interventions . Pediatr Clin North Am . 2016 ; 63 ( 3 ): 389 – 399 .
Naar S . From bench to bedside: T1 translation of basic behavioral science into novel pediatric obesity interventions . Pediatr Clin North Am . 2016 ; 63 ( 3 ): xv – xvi .
Young-Hyman D . Introduction to special issue: self-regulation of appetite – it’s complicated . Obesity (Silver Spring) . 2017 ; 25 ( suppl 1 ): S5 – S7 .
Nielsen L , Riddle M , King JW , et al. ; NIH Science of Behavior Change Implementation Team . The NIH science of behavior change program: transforming the science through a focus on mechanisms of change . Behav Res Ther . 2018 ; 101 : 3 – 11 .
Bryan AD , Jakicic JM , Hunter CM , Evans ME , Yanovski SZ , Epstein LH . Behavioral and psychological phenotyping of physical activity and sedentary behavior: implications for weight management . Obesity (Silver Spring) . 2017 ; 25 ( 10 ): 1653 – 1659 .
Kral TVE, Moore RH, Chittams J, Jones E, O’Malley L, Fisher JO. Identifying behavioral phenotypes for childhood obesity. Appetite. 2018;127:87–96. doi:10.1016/j.appet.2018.04.021
Lumeng JC , Taveras EM , Birch L , Yanovski SZ . Prevention of obesity in infancy and early childhood: a National Institutes of Health workshop . JAMA Pediatr . 2015 ; 169 ( 5 ): 484 – 490 .
Clifton RG , Evans M , Cahill AG , et al. ; LIFE-Moms Research Group . Design of lifestyle intervention trials to prevent excessive gestational weight gain in women with overweight or obesity . Obesity . 2016 ; 24 ( 2 ): 305 – 313 .
Peaceman AM, Clifton RG, Phelan S, et al.; LIFE‐Moms Research Group. Lifestyle interventions limit gestational weight gain in women with overweight or obesity: LIFE-Moms prospective meta-analysis. Obesity . 2018;26(9):1396–1404. doi:10.1002/oby.22250
Gillman MW , Blaisdell CJ . Environmental influences on child health outcomes, a research program of the National Institutes of Health . Curr Opin Pediatr . 2018 ; 30 ( 2 ): 260 – 262 .
Hunter CM , McKinnon RA , Esposito L . News from the NIH: research to evaluate “natural experiments” related to obesity and diabetes . Transl Behav Med . 2014 ; 4 ( 2 ): 127 – 129 .
Institute of Medicine . Bridging the Evidence Gap in Obesity Prevention: A Framework to Inform Decision Making . Washington, DC : The National Academies Press ; 2010 .
The NIH Obesity Research Task Force . Strategic Plan for NIH Obesity Research . NIH Publication No. 11–5493. Bethesda, MD: The National Institutes of Health ; 2011 .
Arteaga SS , Loria CM , Crawford PB , et al. The Healthy Communities Study: its rationale, aims, and approach . Am J Prev Med . 2015 ; 49 ( 4 ): 615 – 623 .
Strauss WJ , Nagaraja J , Landgraf AJ , et al. The longitudinal relationship between community programmes and policies to prevent childhood obesity and BMI in children: the Healthy Communities Study . Pediatr Obes . 2018 . Epub ahead of print. doi: 10.1111/ijpo.12266
Pratt CA , Arteaga S , Loria C . Forging a future of better cardiovascular health: addressing childhood obesity . J Am Coll Cardiol . 2014 ; 63 ( 4 ): 369 – 371 .
Pratt CA , Boyington J , Esposito L , et al. Childhood Obesity Prevention and Treatment Research (COPTR): interventions addressing multiple influences in childhood and adolescent obesity . Contemp Clin Trials . 2013 ; 36 ( 2 ): 406 – 413 .
Barkin SV , Heerman WJ , Sommer EC , et al. Effect of a behavioral intervention for underserved preschool-age children on change in body mass index: a randomized clinical trial . JAMA . 2018;320(5):450–460 .
French SA , Sherwood NE , et al. NET-works randomized clinical trial: Results of a three-year childhood obesity prevention intervention for preschool-aged children . Am J Public Health. 2018 July. in press
Pratt CA , Loria CM , Arteaga SS , et al. A systematic review of obesity disparities research . Am J Prev Med . 2017 ; 53 ( 1 ): 113 – 122 .
Stevens J , Pratt C , Boyington J , et al. Multilevel interventions targeting obesity: research recommendations for vulnerable populations . Am J Prev Med . 2017 ; 52 ( 1 ): 115 – 124 .
Krueger PM , Reither EN . Mind the gap: race/ethnic and socioeconomic disparities in obesity . Curr Diab Rep . 2015 ; 15 ( 11 ): 95 .
Writing Group for the National Collaborative on Childhood Obesity Research . A national collaborative for building the field of childhood obesity research . Am J Prev Med . 2018 ; 54 ( 3 ): 453 – 464 .
Kelly AS , Barlow SE , Rao G , et al. ; American Heart Association Atherosclerosis, Hypertension, and Obesity in the Young Committee of the Council on Cardiovascular Disease in the Young, Council on Nutrition, Physical Activity and Metabolism, and Council on Clinical Cardiology . Severe obesity in children and adolescents: identification, associated health risks, and treatment approaches: a scientific statement from the American Heart Association . Circulation . 2013 ; 128 ( 15 ): 1689 – 1712 .
Reedy J , Subar AF , George SM , Krebs-Smith SM . Extending methods in dietary patterns research . Nutrients . 2018 ; 10 ( 5 ) :571.
Mahabir S , Willett WC , Friedenreich CM , et al. Research strategies for nutritional and physical activity epidemiology and cancer prevention . Cancer Epidemiol Biomarkers Prev . 2018 ; 27 ( 3 ): 233 – 244 .
Fatima Y , Doi SA , Mamun AA . Longitudinal impact of sleep on overweight and obesity in children and adolescents: a systematic review and bias-adjusted meta-analysis . Obes Rev . 2015 ; 16 ( 2 ): 137 – 149 .
Miller MA , Kruisbrink M , Wallace J , Ji C , Cappuccio FP . Sleep duration and incidence of obesity in infants, children, and adolescents: a systematic review and meta-analysis of prospective studies . Sleep . 2018 ; 41 ( 4 ). doi:10.1093/sleep/zsy018
Wu Y , Gong Q , Zou Z , Li H , Zhang X . Short sleep duration and obesity among children: a systematic review and meta-analysis of prospective studies . Obes Res Clin Pract . 2017 ; 11 ( 2 ): 140 – 150 .
Hart CN , Hawley NL , Wing RR . Development of a behavioral sleep intervention as a novel approach for pediatric obesity in school-aged children . Sleep Med Clin . 2016 ; 11 ( 4 ): 515 – 523 .
| Month: | Total Views: |
|---|---|
| October 2018 | 648 |
| November 2018 | 301 |
| December 2018 | 104 |
| January 2019 | 80 |
| February 2019 | 126 |
| March 2019 | 218 |
| April 2019 | 269 |
| May 2019 | 413 |
| June 2019 | 64 |
| July 2019 | 42 |
| August 2019 | 117 |
| September 2019 | 427 |
| October 2019 | 708 |
| November 2019 | 641 |
| December 2019 | 359 |
| January 2020 | 423 |
| February 2020 | 488 |
| March 2020 | 425 |
| April 2020 | 421 |
| May 2020 | 283 |
| June 2020 | 362 |
| July 2020 | 394 |
| August 2020 | 323 |
| September 2020 | 573 |
| October 2020 | 584 |
| November 2020 | 639 |
| December 2020 | 354 |
| January 2021 | 394 |
| February 2021 | 590 |
| March 2021 | 579 |
| April 2021 | 599 |
| May 2021 | 371 |
| June 2021 | 270 |
| July 2021 | 240 |
| August 2021 | 229 |
| September 2021 | 299 |
| October 2021 | 369 |
| November 2021 | 328 |
| December 2021 | 222 |
| January 2022 | 169 |
| February 2022 | 242 |
| March 2022 | 196 |
| April 2022 | 216 |
| May 2022 | 160 |
| June 2022 | 132 |
| July 2022 | 98 |
| August 2022 | 129 |
| September 2022 | 131 |
| October 2022 | 172 |
| November 2022 | 167 |
| December 2022 | 117 |
| January 2023 | 124 |
| February 2023 | 140 |
| March 2023 | 99 |
| April 2023 | 124 |
| May 2023 | 109 |
| June 2023 | 53 |
| July 2023 | 49 |
| August 2023 | 39 |
| September 2023 | 59 |
| October 2023 | 51 |
| November 2023 | 44 |
| December 2023 | 44 |
| January 2024 | 47 |
| February 2024 | 60 |
| March 2024 | 52 |
| April 2024 | 65 |
| May 2024 | 29 |
| June 2024 | 35 |
| July 2024 | 44 |
| August 2024 | 37 |
| September 2024 | 10 |
Email alerts
Citing articles via.
- Recommend to Your Librarian
- Advertising & Corporate Services
Affiliations
- Online ISSN 1613-9860
- Print ISSN 1869-6716
- Copyright © 2024 Society of Behavioural Medicine
- About Oxford Academic
- Publish journals with us
- University press partners
- What we publish
- New features
- Open access
- Institutional account management
- Rights and permissions
- Get help with access
- Accessibility
- Advertising
- Media enquiries
- Oxford University Press
- Oxford Languages
- University of Oxford
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
- Copyright © 2024 Oxford University Press
- Cookie settings
- Cookie policy
- Privacy policy
- Legal notice
This Feature Is Available To Subscribers Only
Sign In or Create an Account
This PDF is available to Subscribers Only
For full access to this pdf, sign in to an existing account, or purchase an annual subscription.
- Alzheimer's disease & dementia
- Arthritis & Rheumatism
- Attention deficit disorders
- Autism spectrum disorders
- Biomedical technology
- Diseases, Conditions, Syndromes
- Endocrinology & Metabolism
- Gastroenterology
- Gerontology & Geriatrics
- Health informatics
- Inflammatory disorders
- Medical economics
- Medical research
- Medications
- Neuroscience
- Obstetrics & gynaecology
- Oncology & Cancer
- Ophthalmology
- Overweight & Obesity
- Parkinson's & Movement disorders
- Psychology & Psychiatry
- Radiology & Imaging
- Sleep disorders
- Sports medicine & Kinesiology
- Vaccination
- Breast cancer
- Cardiovascular disease
- Chronic obstructive pulmonary disease
- Colon cancer
- Coronary artery disease
- Heart attack
- Heart disease
- High blood pressure
- Kidney disease
- Lung cancer
- Multiple sclerosis
- Myocardial infarction
- Ovarian cancer
- Post traumatic stress disorder
- Rheumatoid arthritis
- Schizophrenia
- Skin cancer
- Type 2 diabetes
- Full List »
share this!
September 11, 2024
This article has been reviewed according to Science X's editorial process and policies . Editors have highlighted the following attributes while ensuring the content's credibility:
fact-checked
trusted source
Rapid control of blood sugar levels in gestational diabetes can reverse risk of children developing obesity
by Diabetologia

Swiftly achieving glycemic control after a diagnosis of gestational diabetes can bring the baby's risk of obesity in childhood down to a level similar to that of children whose mothers did not have gestational diabetes, according to new research being presented at the annual meeting of the European Association for the Study of Diabetes (EASD) in Madrid, Spain (9-13 September).
Gestational diabetes, a type of diabetes that can develop during pregnancy, affects 14% of pregnant women globally and is becoming more common among those who are living with obesity, who have a family history of diabetes, and/or who are older at greater risk. Race and ethnicity can also affect risk.
It usually goes away after birth but carries a range of risks during and after pregnancy. Mothers are at high risk of developing diabetes a few years later and their children are at higher risk of premature birth, being born with a large-for-gestational-age weight and having neonatal hypoglycemia. Children are also at higher risk of cardiometabolic complications later in life, including obesity and diabetes.
"Achieving glycemic control soon after the diagnosis of gestational diabetes and maintaining it through pregnancy, up to the delivery, is associated with reduced rates of perinatal complications," says lead researcher Dr. Assiamira Ferrara, Director of the Center for Upstream Prevention of Adiposity and Diabetes Mellitus, Division of Research, Kaiser Permanente Northern California, Oakland, California, U.S..
"Treatments, which include healthy diet , exercise and blood-sugar lowering medications, aim to achieve optimal glycemic control—keep blood sugar in the normal range—during pregnancy."
However, the role of glycemic control on child obesity risk has yet to be proven.
To find out more, Dr. Ferrara and colleagues studied 258,064 women who gave birth in the US between 2011 and 2023 and their children.
In total, 17,316 of the women had gestational diabetes and control of their blood sugar after diagnosis was divided into four trajectories or groups: stably in the optimal range (patients who achieved optimal glycemic control soon after diagnosis and maintained it throughout their pregnancy, 39.2%), rapidly improving to optimal (patients who achieved optimal glycemic control within 4-6 weeks of diagnosis and maintained it throughout their pregnancy, 32.3%), slowly improving to near optimal (16.7%) and slowly improving to suboptimal (11.8%).
Childhood obesity was defined as sex-specific BMI-for-age ≥95th percentile, based on the United States Centers for Disease Control and Prevention charts.
Obesity prevalence at 2-4 years was 15.1% in children of women without gestational diabetes, and 15.9%, 18.7%, 20.9% and 24.6% in children of women in the stably optimal, rapidly improving to optimal, slowly improving to near optimal and slowly improving to suboptimal glycemic control groups, respectively.
Further analysis showed that the risk of childhood obesity increased with maternal blood sugar levels.
At 2-4 years, children of women with gestational diabetes in the stably optimal and rapidly improving to optimal groups had a similar risk of obesity to those whose mothers didn't have gestational diabetes.
Children of women with gestational diabetes in the slowly improving to near optimal and slowly improving to suboptimal groups had a higher risk of obesity (13% and 23% higher, respectively).
At 5-7 years, only children of women with gestational diabetes in the stably optimal group had an obesity risk similar to that observed in children of individuals without gestational diabetes.
The children whose mothers were in the rapidly improving to optimal and slowly improving to near optimal were at 18% and 19% higher risk of childhood obesity, respectively, than those whose mothers didn't have gestational diabetes.
For those whose mothers blood sugar was the least well controlled, the slowly improving to suboptimal group, the risk of childhood obesity was 30% higher.
The study's authors conclude that swiftly achieving glycemic control after diagnosis of gestational diabetes can bring the childhood obesity risk down to a level similar to that seen in children whose mothers did not have gestational diabetes.
Dr. Ferrara says, "When gestational diabetes is not properly managed, this increases the baby's risk of a high birth weight and may predispose them to obesity. The good news is that if the mother's blood sugar is quickly brought under control, her baby's risk of childhood obesity is similar to that of children whose mothers had normal blood sugar in pregnancy.
"Women who are diagnosed with gestational diabetes should start to follow the treatment plan drawn up by their physician as soon as possible. This is likely to initially involve dietary changes, exercise and monitoring of glucose levels. If blood sugar levels are not in the recommended range within two weeks, they should start medication to lower the level, as prescribed.
"Obesity increases the risk of developing diabetes and heart disease , and once it is established, it is hard to reverse, and so anything we can do to reduce the risk of it developing is important."
Explore further
Feedback to editors

Long-term metastatic melanoma survival dramatically improves on immunotherapy, clinical trial finds
22 minutes ago

Team discovers role of ferroptosis in combating breast cancer resistance
Sep 13, 2024

Metformin found to reduce organ aging in male monkeys

Researchers discover new target for treating heart failure: Protein kinase N

RNA-sequencing study provides novel insights into chronic lymphocytic leukemia

Scientists discover potential cause of an enigmatic vascular disease primarily impacting women

Key factors identified that can impact long-term weight loss in patients with obesity prescribed GLP-1 RA medications

Study finds 'supercharging' T cells with mitochondria enhances their antitumor activity

Using AI, researchers find e-cigarette brands are skirting the rules about health warning labels on Instagram

New therapy that targets and destroys tau tangles: A promising Alzheimer's disease treatment
Related stories.

Higher blood sugar level at gestational diabetes diagnosis linked to harmful outcomes for mothers and babies
May 13, 2024

Researchers quantify the risk for diabetes after gestational diabetes
May 10, 2024

Gestational diabetes does not increase risk of breast cancer, large Danish study finds
Aug 6, 2024

Pregnant women with obesity and diabetes may be more likely to have a child with ADHD
Sep 8, 2022

Early control of blood sugar key for gestational diabetes
Sep 29, 2022

Pregnant mom's high blood sugar affects kids at ages 10 to 14
Jan 21, 2019
Recommended for you

Automated insulin delivery technology helps marathon runners with type 1 diabetes
Sep 12, 2024

Exposure to air pollution during pregnancy increases postpartum depression risk for at least three years, study finds

Stress-induced events jumpstart sperm performance once the event has passed, research reveals
Sep 11, 2024

Implanting aged oocytes in young follicles can produce rejuvenated eggs, researchers find

Sterilization rates among women rose after Supreme Court abortion ruling, study finds

Unaffordable food putting moms-to-be at risk, research shows
Sep 10, 2024
Let us know if there is a problem with our content
Use this form if you have come across a typo, inaccuracy or would like to send an edit request for the content on this page. For general inquiries, please use our contact form . For general feedback, use the public comments section below (please adhere to guidelines ).
Please select the most appropriate category to facilitate processing of your request
Thank you for taking time to provide your feedback to the editors.
Your feedback is important to us. However, we do not guarantee individual replies due to the high volume of messages.
E-mail the story
Your email address is used only to let the recipient know who sent the email. Neither your address nor the recipient's address will be used for any other purpose. The information you enter will appear in your e-mail message and is not retained by Medical Xpress in any form.
Newsletter sign up
Get weekly and/or daily updates delivered to your inbox. You can unsubscribe at any time and we'll never share your details to third parties.
More information Privacy policy
Donate and enjoy an ad-free experience
We keep our content available to everyone. Consider supporting Science X's mission by getting a premium account.
E-mail newsletter
Influence of local geological data and geographical parameters to assess regional health impact in LCA. Tomsk oblast’, Russian Federation application case
- Research Article
- Published: 08 July 2022
- Volume 29 , pages 87281–87297, ( 2022 )
Cite this article

- Alexandra Belyanovskaya ORCID: orcid.org/0000-0003-4320-7637 1 , 2 ,
- Bulat Soktoev 1 ,
- Bertrand Laratte 3 ,
- Elena Ageeva 1 ,
- Natalia Baranovskaya 1 &
- Natalia Korogod 4
319 Accesses
2 Citations
Explore all metrics
The research paper is aimed to modify the human health impact assessment of Cr in soils. The current article presents the input of several critical parameters for the human health Impact Score (IS hum ) assessment in soils. The modification of the IS hum is derived using geological data — results of neutron activation analysis of soils are used in the IS hum calculation; research area is divided using the watersheds and population size and density. Watersheds reflect the local environmental conditions of the territory unlike the administrative units (geographical areas of the studied region) due to their geological independence. The calculations of the characterization factor value underestimate the influence of the population size and density on the final result. Default characterization factor values cannot be considered during the assessment of the potential human health impact for the big sparsely inhabited areas. In case of very low population density, the result will be overrated and underestimated in the opposite case. The current approach demonstrates that the geographical separation in the USEtox model should be specified. The same approach can be utilized for other geo zones due to the accessibility of this information (area size, population size, and density, geological, and landscape features).
This is a preview of subscription content, log in via an institution to check access.
Access this article
Subscribe and save.
- Get 10 units per month
- Download Article/Chapter or eBook
- 1 Unit = 1 Article or 1 Chapter
- Cancel anytime
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
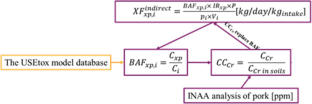
Similar content being viewed by others

Depth of the pedological profile as a conditioning factor of soil erodibility (RUSLE K-Factor) in Ecuadorian basins
Soil erodibility mapping using the rusle model to prioritize erosion control in the wadi sahouat basin, north-west of algeria, a spatially explicit life cycle assessment midpoint indicator for soil quality in the european union using soil organic carbon, explore related subjects.
- Environmental Chemistry
Author information
Authors and affiliations.
Division for Geology at Tomsk Polytechnic University, Tomsk, Russia
Alexandra Belyanovskaya, Bulat Soktoev, Elena Ageeva & Natalia Baranovskaya
Laboratory of Sedimentology and Paleobiosphere Evolution, Tyumen, Russia
Alexandra Belyanovskaya
Arts et Métiers Institute of Technology, University of Bordeaux, CNRS, Bordeaux INP, INRAE, I2M, Bordeaux, F-33400 Talence, France
Bertrand Laratte
High School of Natural Science at Pavlodar State Pedagogical University, Pavlodar, Kazakhstan
Natalia Korogod
You can also search for this author in PubMed Google Scholar
Contributions
Alexandra I. Belyanovskaya: Conceptualization, Data curation, Writing - original draft, Formal analysis.
Bulat R. Soktoev: Writing - original draft, Formal analysis.
Bertrand Laratte: Conceptualization, Supervision, Methodology.
Elena V. Ageeva: Writing - original draft, Formal analysis.
Natalia V. Baranovskaya: Conceptualization, Supervision.
Natalia P. Korogod: Conceptualization.
Corresponding author
Correspondence to Alexandra Belyanovskaya .
Ethics declarations
Ethics approval.
The authors declare that all applicable international, national, and institutional guidelines for the care and use of animals were followed. Sampling of biomaterial was carried out as part of the slaughter of the livestock in a private farm.
Consent to participate
Not applicable.
Consent for publication
Competing interests.
The authors declare no competing interests.
Additional information
Responsible Editor: Philippe Loubet
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
(DOCX 44 kb)
Rights and permissions
Reprints and permissions
About this article
Belyanovskaya, A., Soktoev, B., Laratte, B. et al. Influence of local geological data and geographical parameters to assess regional health impact in LCA. Tomsk oblast’, Russian Federation application case. Environ Sci Pollut Res 29 , 87281–87297 (2022). https://doi.org/10.1007/s11356-022-21784-9
Download citation
Received : 26 November 2021
Accepted : 28 June 2022
Published : 08 July 2022
Issue Date : December 2022
DOI : https://doi.org/10.1007/s11356-022-21784-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Heavy metals
- Regional impact assessment
- Impact assessment models
- Find a journal
- Publish with us
- Track your research
Are playgrounds too safe? Why anthropologists say kids need to monkey around
Trying to make playgrounds safer can do more harm than good, experts say.

Social Sharing
Raise your hand if you've ever fallen off the monkey bars and hurt more than your pride.
It's practically a childhood rite of passage. You climb, you swing, you push the limit, you miss, you cry. Maybe you dusted yourself off and limped back onto the playground. Or maybe you needed a trip to the emergency room to have a bone reset. (But if you were lucky, the cast came off in time to still enjoy some late-summer swimming).
Monkey bars, jungle gyms and playgrounds are synonymous with childhood play. They are also often the target of campaigns to reduce risk, sometimes get torn down due to safety concerns, and are often redesigned to be as injury-proof as possible.
Yet a new report from a team of anthropologists from Dartmouth College in Hanover, N.H., argues that these iconic play structures exercise a biological need passed down from apes that may be critical to childhood development. And the authors say well-intentioned efforts to mitigate their risk may, in fact, be harming kids.
In August, the authors wrote in the journal Evolution, Medicine, and Public Health that primates learn to climb at a young age to find food, stay safe from predators and to sleep in the branches of trees. So it's little wonder that children have a natural proclivity to climb and explore.
In other words, there's a reason they're called monkey bars.
"Climbing is a part of us. We have been climbing for millions of years," lead author Luke Fannin, a PhD candidate in the ecology, evolution, environment and society program at Dartmouth College, told CBC News.

Playgrounds provide a necessary challenge for children to build confidence, take calculated risks and test boundaries, Fannin said. And while children do sometimes get hurt on them, we need to strike a delicate balance between statistical risk and biological reward.
"We're not saying that playgrounds shouldn't be regulated," Fannin said.
"But we need to make playgrounds as safe as necessary, not as safe as possible."
Risk versus reward
Childhood injuries remain a major public health issue according to a 2023 report from the Public Health Agency of Canada. The report, using self-reported data from the 2019 Canadian Health Survey on Children and Youth, said unintentional injuries are the leading cause of death among Canadian children and youth.
Head injuries were the most commonly reported injuries in children, according to the report, but it also noted that children were more likely to require medical treatment for injuries related to sports and physical activity than for injuries related to playing.
Children do get injured using playground equipment — most typically, bone fractures — but kids can usually recover fully from these injuries, and overall, the risk is low, says Pamela Fuselli, the president and CEO of safety advocacy group Parachute Canada, who was not involved with the anthropological research.

The key to healthy kids is risky outdoor play, researchers say
It's about balance, she said — softer play surfaces and lower play structures have helped reduce injuries over the years, but "we also don't want to take the fun out of play for all ages."
"We need to loosen the reins a little bit," Fuselli said.
Melanie Quilty, a mother of twin eight-year-olds in Kingston, Ont., says she agrees safety measures have swung too far.
"We have to teach them to do these dangerous things safely ... teach them confidence, and to trust their instincts," said Quilty, who works in health care.
Last year, her son, Conner, fell off the monkey bars at a park and broke his arm. He needed surgery and wore a cast for about eight weeks. But Quilty, 40, says she wasn't nervous about him getting back on the bars when his cast came off — she was more nervous he wouldn't want to.
"I don't want him to be afraid his whole life," she said.

How modern parenting plays a role
In January, the Canadian Paediatric Society (CPS) released new guidelines emphasizing the importance of unstructured outdoor play for children's development and physical and mental health amid rising obesity, anxiety and behavioural issues.
In its guidelines, CPS argued that kids today have fewer opportunities to engage in risky outdoor play, and that's in part because of safety measures that "have sought to prevent all play-related injuries rather than focusing on serious and fatal injuries."
Modern parental anxiety plays into our unwillingness to let children take risks despite the developmental benefits, Fannin says.
In the last 100 years, modern parenting has shifted from a community to individual approach, he said. This creates pressure on parents to keep their own kids safe, which he describes in the paper as a "modern moral imperative."

Flipping out over Calgary's new parkour playground
Parents today are also constantly inundated with information and comparisons thanks to social media and smartphones, the U.S. Surgeon General wrote in a public health advisory earlier in September about the pressures of modern parenting.
In other words, if a child is injured in an accident on the other side of the planet, parents today are more likely to hear about it. At the same time, parents today may worry about judgment if they post a photo of their child in a cast on Instagram.
- Pop the bubble wrap and let kids play outdoors, pediatricians say
- Modern parenting is so stressful that the U.S. issued a health advisory. Parents say it's overdue
Yet, in many ways, children have never been physically safer. Crime rates have been on a downward trend since the 1990s, when many of today's modern parents were children themselves (and may have formed some core memories of missing kids on milk cartons and stranger danger).
Today, there are laws for car seats, seat belts and bike helmets. You can put an AirTag on your kid and know where they are at any given time.
Are playgrounds too boring?
In its January recommendations, CPS cited 2011-23 data from the Canadian Hospital Injury Reporting and Prevention Program on injury types sustained during popular childhood activities. The injury rate of falls from playground equipment was 4,090 cases per 100,000 — slightly lower than the rate of injury from playing soccer.
"Some experts have attributed playground injuries to unexciting play structures," CPS wrote in the report, explaining that structures that are too boring may lead to kids using the equipment inappropriately and take greater risks.

Jungle gyms and monkey bars are about 100 years old — patented in 1923 and 1924 by U.S. lawyer Sebastian "Ted" Hinton. Even Hinton, in his first patent , noted the link to primates.
"Climbing is the natural method of locomotion which the evolutionary predecessors of the human race were designed to practice, and is therefore almost ideally suited for children," he wrote.
- LISTEN Pediatricians say kids need 'risky play.' Parents, take a deep breath
- Which generation of parents had it the hardest? It depends who you ask
Much has changed since the earliest jungle gyms, which were, essentially, a grid of metal poles. As NPR notes, safety concerns have "softened materials and rounded edges." Smithsonian Magazine explained there was a rise of "ultra-safe" playgrounds in the 1990s designed to minimize harm.
Fuselli, with Parachute Canada, says she thinks that the focus on making playgrounds safer has gone too far. And she knows that sentiment flies in the face of injury prevention.
"But there's a risk to everything," she said. And when you balance the low risk of serious injury on playgrounds with the risks of children not playing — like higher risks of obesity, and the risk of online harms — it makes sense, she added.
"You know, a child going down the street to play at the playground — the actual risk is more around the street than anything else."

ABOUT THE AUTHOR

Senior Writer & Editor
Natalie Stechyson has been a writer and editor at CBC News since 2021. She covers stories on social trends, families, gender, human interest, as well as general news. She's worked as a journalist since 2009, with stints at the Globe and Mail and Postmedia News, among others. Before joining CBC News, she was the parents editor at HuffPost Canada, where she won a silver Canadian Online Publishing Award for her work on pregnancy loss. You can reach her at [email protected].
Related Stories
- When bats were wiped out, more human babies died, a study found. Here's why
- Should parents of boys set aside the topic of toxic masculinity? This author thinks so
- Orangutan briefly escapes outdoor habitat at Toronto Zoo
- Residents use 'tactical urbanism' to ward off overcrowding at inner-city parks
Academia.edu no longer supports Internet Explorer.
To browse Academia.edu and the wider internet faster and more securely, please take a few seconds to upgrade your browser .
Enter the email address you signed up with and we'll email you a reset link.
- We're Hiring!
- Help Center

A pilot screening of prevalence of atopic states and opisthorchosis and their relationship in people of Tomsk Oblast

2007, Parasitology Research
Related Papers
Public Health Open Access
stephen aremu
Introduction: Opisthorchiasis is no doubt one of the most neglected infectious disease inspite of its huge medical importance in some parts of the World. The past decade have seen a resurgence of interests in research relating to this public health issue, however there is still a lot to be done. Social Model: Not many models have been explored in Western Siberia to deal with the opisthorchiasis epidemic when compared to the different models that have been used for other regions affected by similar disease. Life Cycle: The complex life cycle of Opisthorchis felineus has humans and other feline species as definitive host and is really prevalent among the aboriginal population of the Western Siberian because of their habit of eating raw or undercooked fresh water fish (Cyprinidae) which are intermediate host of the parasite. Diagnosis and Treatment: Diagnosis involve the use of stool microscopy, other methods such as mAb ELISA, LAMP and so on are used, while the common treatment is the...
Charlotte Braun-fahrländer
World Allergy Organization Journal
Maria Prisco
Izabela Kupryś-Lipińska
Introduction: A dramatic increase in the prevalence of atopic diseases can be observed. The reasons for this phenomenon remain unclear. Aim: To compare the prevalence of atopic diseases in subjects living in the city centre and a rural area. Material and methods: The study was done on a randomly chosen group of inhabitants of Lodz province, aged 3 to 80 years, living in two different areas: the city centre and a rural area. Demographic data and the anamnesis were collected on the basis of standardised questionnaires. Additionally, skin prick tests and screening spirometries were performed. Results: The complete data from 482 subjects living in the city centre and 469 in the rural area were included in the analysis. Asthma prevalence in the city centre was estimated at 13.2% in adults and 18.4% in children compared to 4.2 and 6.0% respectively in the rural area. The prevalence of seasonal allergic rhinitis in the city centre was 13.2% in adults and 16.1% in children, in comparison to...
Online journal of biological sciences
Alexandra Tegza
Clinical & Experimental Allergy
Silver Siiak
Journal of Parasitic Diseases
Amin Ahmadi
PLoS Neglected Tropical Diseases
Hafizatul Zan
Suez Canal Veterinary Medical Journal. SCVMJ
Eman Youssef
Loading Preview
Sorry, preview is currently unavailable. You can download the paper by clicking the button above.
RELATED PAPERS
Adnan Custovic
Veterinary World
Veterinary World , Dmitry Podshibyakin
Parasitology Research
Menelaos Lefkaditis
The Korean Journal of Parasitology
Dr. Qais Majeed
Nina A Samoylovskaya
International Archives of Allergy and Immunology
Johannes Ring
Georgiana Deak
Heri Wibowo
Pediatric Allergy and Immunology
Helminthologia
Vasile Cozma
Croatian Medical Journal
Lucija Buneta
Veterinary Parasitology: Regional Studies and Reports
Christina Loftin
Journal of Allergy and Clinical Immunology
Laura Rodrigues
Iranian journal of parasitology
Nasser Hajipour
Acta Tropica
Paiboon Sithithaworn
Tropical medicine and health
Kazuhiko Moji
Environment and Pollution
Barbara Kołłątaj
İrfan Şencan
ricardo lopez
Turkish Journal of Veterinary & Animal Sciences
Nurainie Ismail
Elpis Mantadakis
Jane Hoppin
Emerging Infectious …
Teresa Bossù
RELATED TOPICS
- We're Hiring!
- Help Center
- Find new research papers in:
- Health Sciences
- Earth Sciences
- Cognitive Science
- Mathematics
- Computer Science
- Academia ©2024
An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- J Family Med Prim Care
- v.4(2); Apr-Jun 2015
Childhood obesity: causes and consequences
Krushnapriya sahoo.
1 Phd Scholar, Department of Human Development and Family Studies, Maharana Pratap University of Agriculture and Technology, Udaipur, Rajasthan, India
Bishnupriya Sahoo
2 Senior Resident, Department of Pediatrics, Vardhmann Medical College and Safdarjung Hospital, New Delhi, India
Ashok Kumar Choudhury
3 Assistant Professor, Department of Hepatology, Institute of Liver and Biliary Sciences, New Delhi, India
Nighat Yasin Sofi
4 Research Scientist, Human Nutrition Unit, All India Institute of Medical Sciences, New Delhi, India
Raman Kumar
5 CMO In Charge Emergency, Department of Clinical Research, Institute of Liver and Biliary Sciences, New Delhi, India
Ajeet Singh Bhadoria
6 Epidemiologist and Public Health Specialist, Department of Clinical Research, Institute of Liver and Biliary Sciences, New Delhi, India
Childhood obesity has reached epidemic levels in developed as well as in developing countries. Overweight and obesity in childhood are known to have significant impact on both physical and psychological health. Overweight and obese children are likely to stay obese into adulthood and more likely to develop non-communicable diseases like diabetes and cardiovascular diseases at a younger age. The mechanism of obesity development is not fully understood and it is believed to be a disorder with multiple causes. Environmental factors, lifestyle preferences, and cultural environment play pivotal roles in the rising prevalence of obesity worldwide. In general, overweight and obesity are assumed to be the results of an increase in caloric and fat intake. On the other hand, there are supporting evidence that excessive sugar intake by soft drink, increased portion size, and steady decline in physical activity have been playing major roles in the rising rates of obesity all around the world. Childhood obesity can profoundly affect children's physical health, social, and emotional well-being, and self esteem. It is also associated with poor academic performance and a lower quality of life experienced by the child. Many co-morbid conditions like metabolic, cardiovascular, orthopedic, neurological, hepatic, pulmonary, and renal disorders are also seen in association with childhood obesity.
Introduction
The world is undergoing a rapid epidemiological and nutritional transition characterized by persistent nutritional deficiencies, as evidenced by the prevalence of stunting, anemia, and iron and zinc deficiencies. Concomitantly, there is a progressive rise in the prevalence of obesity, diabetes and other nutrition related chronic diseases (NRCDs) like obesity, diabetes, cardiovascular disease, and some forms of cancer. Obesity has reached epidemic levels in developed countries. The highest prevalence rates of childhood obesity have been observed in developed countries; however, its prevalence is increasing in developing countries as well.[ 1 ] Females are more likely to be obese as compared to males, owing to inherent hormonal differences.[ 2 ]
It is emerging convincingly that the genesis of Type 2 Diabetes and Coronary Heart Disease begins in childhood, with childhood obesity serving as an important factor.[ 3 ] There has been a phenomenal rise in proportions of children having obesity in the last 4 decades, especially in the developed world. Studies emerging from different parts of India within last decade are also indicative of similar trend.[ 4 , 5 , 6 , 7 , 8 , 9 ] This view has been challenged over recent years and we presently consider these as different forms of the global malnutrition problem. This new conceptualization leads us to simultaneously address the root causes of nutritional deficiencies which in turn will contribute to the control of under nutrition and the prevention of obesity, diabetes, and other NRCDs. This summary provides a public health overview of selected key issues related to the prevention of obesity and chronic diseases with a life-course perspective of nutrition and child growth.
Childhood obesity is one of the most serious public health challenges of the 21 st century. The problem is global and is steadily affecting many low and middle income countries, particularly in urban settings. The prevalence has increased at an alarming rate. Globally in 2010, the number of overweight children under the age of five is estimated to be over 42 million. Close to 35 million of these are living in developing countries.
Definition of Childhood Obesity
Although definition of obesity and overweight has changed over time, it can be defined as an excess of body fat (BF). There is no consensus on a cut-off point for excess fatness of overweight or obesity in children and adolescents. A study by conducted by Williams et al . (1992), on 3,320 children in the age-group of 5–18 years classified children as fat if their percentage of body fat was at least 25% for males and 30% for females, respectively.[ 10 ] The Center for Disease Control and Prevention defined overweight as at or above the 95 th percentile of body mass index (BMI) for age and “at risk for overweight” as between 85 th to 95 th percentile of BMI for age.[ 11 , 12 ] European researchers classified overweight as at or above 85 th percentile and obesity as at or above 95 th percentile of BMI.[ 13 ]
An Indian research study has defined overweight and obesity as overweight (between ≥85 th and <95 th percentile) and obesity (≥95 th percentile).[ 14 ] Another study has followed World Health Organization 2007 growth reference for defining overweight and obesity.[ 15 ]
There are also several methods to measure the percentage of body fat. In research, techniques include underwater weighing (densitometry), multi-frequency bioelectrical impedance analysis (BIA), and magnetic resonance imaging (MRI). In the clinical environment, techniques such as BMI, waist circumference, and skin-fold thickness have been used extensively. Although, these methods are less accurate than research methods, they are satisfactory to identify risk. While BMI seems appropriate for differentiating adults, it may not be as useful in children because of their changing body shape as they progress through normal growth. In addition, BMI fails to distinguish between fat and fat-free mass (muscle and bone) and may exaggerate obesity in large muscular children. Furthermore, maturation pattern differs between genders and different ethnic groups. Studies that used BMI to identify overweight and obese children based on percentage of body fat have found high specificity (95–100%), but low sensitivity (36–66%) for this system of classification.[ 16 ] While health consequences of obesity are related to excess fatness, the ideal method of classification should be based on direct measurement of fatness. Although methods such as densitometry can be used in research practice, they are not feasible for clinical settings. For large population-based studies and clinical situations, bioelectrical impedance analysis (BIA) is widely used. Waist circumference seems to be more accurate for children because it targets central obesity, which is a risk factor for type II diabetes and coronary heart disease.
Causes of Childhood Obesity
It is widely accepted that increase in obesity results from an imbalance between energy intake and expenditure, with an increase in positive energy balance being closely associated with the lifestyle adopted and the dietary intake preferences. However, there is increasing evidence indicating that an individual's genetic background is important in determining obesity risk. Research has made important contributions to our understanding of the factors associated with obesity. The ecological model, as described by Davison et al ., suggests that child risk factors for obesity include dietary intake, physical activity, and sedentary behavior.[ 17 ] The impact of such risk factors is moderated by factors such as age, gender. Family characteristics parenting style, parents’ lifestyles also play a role. Environmental factors such as school policies, demographics, and parents’ work-related demands further influence eating and activity behaviors.
Genetics are one of the biggest factors examined as a cause of obesity. Some studies have found that BMI is 25–40% heritable.[ 18 ] However, genetic susceptibility often needs to be coupled with contributing environmental and behavioral factors in order to affect weight.[ 19 ] The genetic factor accounts for less than 5% of cases of childhood obesity.[ 18 ] Therefore, while genetics can play a role in the development of obesity, it is not the cause of the dramatic increase in childhood obesity.
Basal metabolic rate has also been studied as a possible cause of obesity. Basal metabolic rate, or metabolism, is the body's expenditure of energy for normal resting functions. Basal metabolic rate is accountable for 60% of total energy expenditure in sedentary adults. It has been hypothesized that obese individuals have lower basal metabolic rates. However, differences in basal metabolic rates are not likely to be responsible for the rising rates of obesity.[ 18 ]
Review of the literature investigates factors behind poor diet and offers numerous insights into how parental factors may impact on obesity in children.[ 20 ] They note that children learn by modeling parents’ and peers’ preferences, intake and willingness to try new foods. Availability of, and repeated exposure to, healthy foods is key to developing preferences and can overcome dislike of foods. Mealtime structure is important with evidence suggesting that families who eat together consume more healthy foods. Furthermore, eating out or watching TV while eating is associated with a higher intake of fat. Parental feeding style is also significant. The author's found that authoritative feeding (determining which foods are offered, allowing the child to choose, and providing rationale for healthy options) is associated with positive cognitions about healthy foods and healthier intake. Interestingly authoritarian restriction of “junk-food” is associated with increased desire for unhealthy food and higher weight.[ 21 ]
Government and social policies could also potentially promote healthy behavior. Research indicates taste, followed by hunger and price, is the most important factor in adolescents snack choices.[ 22 ] Other studies demonstrate that adolescents associate junk food with pleasure, independence, and convenience, whereas liking healthy food is considered odd.[ 23 ] This suggests investment is required in changing meanings of food, and social perceptions of eating behavior. As proposed by the National Taskforce on Obesity (2005), fiscal policies such as taxing unhealthy options, providing incentives for the distribution of inexpensive healthy food, and investing in convenient recreational facilities or the esthetic quality of neighborhoods can enhance healthy eating and physical activity.[ 24 ]
Dietary factors have been studied extensively for its possible contributions to the rising rates of obesity. The dietary factors that have been examined include fast food consumption, sugary beverages, snack foods, and portion sizes.
Fast food Consumption: Increased fast food consumption has been linked with obesity in the recent years. Many families, especially those with two parents working outside the home, opt for these places as they are often favored by their children and are both convenient and inexpensive.[ 25 ] Foods served at fast food restaurants tend to contain a high number of calories with low nutritional values. A study conducted examined the eating habits of lean and overweight adolescents at fast food restaurants.[ 26 ] Researchers found that both groups consumed more calories eating fast food than they would typically in a home setting but the lean group compensated for the higher caloric intake by adjusting their caloric intake before or after the fast food meal in anticipation or compensation for the excess calories consumed during the fast food meal. Though many studies have shown weight gain with regular consumption of fast food, it is difficult to establish a causal relationship between fast food and obesity.
Sugary beverages
A study examining children aged 9–14 from 1996–1998, found that consumption of sugary beverages increased BMI by small amounts over the years.[ 18 ] Sugary drinks are another factor that has been examined as a potential contributing factor to obesity. Sugary drinks are often thought of as being limited to soda, but juice and other sweetened beverages fall into this category. Many studies have examined the link between sugary drink consumption and weight and it has been continually found to be a contributing factor to being overweight.[ 18 ] Sugary drinks are less filling than food and can be consumed quicker, which results in a higher caloric intake.[ 19 ]
Snack foods
Another factor that has been studied as a possible contributing factor of childhood obesity is the consumption of snack foods. Snack foods include foods such as chips, baked goods, and candy. Many studies have been conducted to examine whether these foods have contributed to the increase in childhood obesity. While snacking has been shown to increase overall caloric intake, no studies have been able to find a link between snacking and overweight.[ 18 ]
Portion size
Portion sizes have increased drastically in the past decade. Consuming large portions, in addition to frequent snacking on highly caloric foods, contribute to an excessive caloric intake. This energy imbalance can cause weight gain, and consequently obesity.[ 18 ]
Activity level
One of the factors that is most significantly linked to obesity is a sedentary lifestyle. Each additional hour of television per day increased the prevalence of obesity by 2%.[ 18 ] Television viewing among young children and adolescents has increased dramatically in recent years.[ 18 , 27 ] The increased amount of time spent in sedentary behaviors has decreased the amount of time spent in physical activity. Research which indicates the number of hours children spend watching TV correlates with their consumption of the most advertised goods, including sweetened cereals, sweets, sweetened beverages, and salty snacks.[ 22 ] Despite difficulties in empirically assessing the media impact, other research discussed emphasizes that advertising effects should not be underestimated. Media effects have been found for adolescent aggression and smoking and formation of unrealistic body ideals. Regulation of marketing for unhealthy foods is recommended, as is media advocacy to promote healthy eating.
Environmental factors
While extensive television viewing and the use of other electronic media has contributed to the sedentary lifestyles, other environmental factors have reduced the opportunities for physical activity. Opportunities to be physically active and safe environments to be active in have decreased in the recent years. The majority of children in the past walked or rode their bike to school. A study conducted in 2002 found that 53% of parents drove their children to school.[ 18 ] Of these parents, 66% said they drove their children to school since their homes were too far away from the school. Other reasons parents gave for driving their children to school included no safe walking route, fear of child predators, and out of convenience for the child.[ 18 ] Children who live in unsafe areas or who do not have access to safe, well-lit walking routes have fewer opportunities to be physically active.[ 18 ]
Socio-cultural factors
Socio-cultural factors have also been found to influence the development of obesity. Our society tends to use food as a reward, as a means to control others, and as part of socializing.[ 28 ] These uses of food can encourage the development of unhealthy relationships with food, thereby increasing the risk of developing obesity.
Family factors
Family factors have also been associated with the increase of cases of obesity. The types of food available in the house and the food preferences of family members can influence the foods that children eat. In addition, family mealtimes can influence the type of food consumed and the amount thereof. Lastly, family habits, whether they are sedentary or physically active, influence the child.[ 28 ] Studies have shown that having an overweight mother and living in a single parent household are associated with overweight and childhood obesity.[ 29 ]
Psychological factors
Depression and anxiety.
A recent review concluded that the majority of studies find a prospective relationship between eating disturbances and depression.[ 30 ] However, this relationship is not unidirectional; depression may be both a cause and a consequence of obesity.[ 31 ] Additionally, in a clinical sample of obese adolescents, a higher life-time prevalence of anxiety disorders was reported compared to non-obese controls.[ 32 ] Although some studies demonstrate no significant relationship between increased BMI and increased anxiety symptoms.[ 33 ] Thus, the relationship between obesity and anxiety may not be unidirectional and is certainly not conclusive.
Self-esteem
Research findings comparing overweight/obese children with normal-weight children in regards to self-esteem have been mixed.[ 34 ] Some studies have found that obese children have lower self-esteem while others do not.[ 35 , 36 , 37 ] There is some consensus in the literature that the global approach to self-esteem measurement with children who are overweight/obese is misleading as the physical and social domains of self-esteem seem to be where these children are most vulnerable.[ 38 ]
Body dissatisfaction
Research has consistently found that body satisfaction is higher in males than females at all ages.[ 39 ] Gender differences may reflect the westernized cultural ideals of beauty in that thinness is the only culturally defined ideal for females, while males are encouraged to be both lean and muscular. Thus, there is a linear relationship between body dissatisfaction and increasing BMI for girls; while for boys a U-shaped relationship suggests that boys with BMIs at the low and high extremes experience high levels of body dissatisfaction.[ 40 , 41 ]
Eating disorder symptoms
Traits associated with eating disorders appear to be common in adolescent obese populations, particularly for girls.[ 42 ] A number of studies have shown higher prevalence of eating-related pathology (i.e. Anorexia, Bulimia Nervosa, and impulse regulation) in obese children/youth.[ 43 , 44 ]
Emotional problems
In one of the few studies to investigate the psychological impact of being overweight/obese in children, a review of 10 published studies over a 10-year period (1995-2005) with sample sizes greater than 50 revealed that all participants reported some level of psychosocial impact as a result of their weight status.[ 45 ] Being younger, female, and with an increased perceived lack of control over eating seemed to heighten the psychosocial consequences.
Consequences of childhood obesity
Childhood obesity can profoundly affect children's physical health, social, and emotional well-being, and self esteem. It is also associated with poor academic performance and a lower quality of life experienced by the child. These potential consequences are further examined in the following sections.
Medical consequences
Childhood obesity has been linked to numerous medical conditions. These conditions include, but are not limited to, fatty liver disease, sleep apnea, Type 2 diabetes, asthma, hepatic steatosis (fatty liver disease), cardiovascular disease, high cholesterol, cholelithiasis (gallstones), glucose intolerance and insulin resistance, skin conditions, menstrual abnormalities, impaired balance, and orthopedic problems.[ 25 , 46 ] Until recently, many of the above health conditions had only been found in adults; now they are extremely prevalent in obese children. Although most of the physical health conditions associated with childhood obesity are preventable and can disappear when a child or adolescent reaches a healthy weight, some continue to have negative consequences throughout adulthood.[ 46 ] In the worst cases, some of these health conditions can even result in death. Below, three of the more common health problems associated with childhood obesity are discussed, diabetes, sleep apnea, and cardiovascular disease.
Socio-emotional consequences
In addition to being implicated in numerous medical concerns, childhood obesity affects children's and adolescent's social and emotional health. Obesity has been described as being “one of the most stigmatizing and least socially acceptable conditions in childhood.”[ 38 ] Overweight and obese children are often teased and/or bullied for their weight. They also face numerous other hardships including negative stereotypes, discrimination, and social marginalization.[ 46 ] Discrimination against obese individuals has been found in children as young as 2 years old.[ 28 ] Obese children are often excluded from activities, particularly competitive activities that require physical activity. It is often difficult for overweight children to participate in physical activities as they tend to be slower than their peers and contend with shortness of breath.[ 25 ] These negative social problems contribute to low self esteem, low self confidence, and a negative body image in children and can also affect academic performance.[ 46 ] All of the above-mentioned negative effects of overweight and obesity can be devastating to children and adolescents.
The social consequences of obesity may contribute to continuing difficulty in weight management. Overweight children tend to protect themselves from negative comments and attitudes by retreating to safe places, such as their homes, where they may seek food as a comfort. In addition, children who are overweight tend to have fewer friends than normal weight children, which results in less social interaction and play, and more time spent in sedentary activities.[ 25 ] As aforementioned, physical activity is often more difficult for overweight and obese children as they tend to get shortness of breath and often have a hard time keeping up with their peers. This in turn inevitably results in weight gain, as the amount of calories consumed exceeds the amount of energy burned.[ 25 ]
Academic consequences
Childhood obesity has also been found to negatively affect school performance. A research study concluded that overweight and obese children were four times more likely to report having problems at school than their normal weight peers.[ 38 ] They are also more likely to miss school more frequently, especially those with chronic health conditions such as diabetes and asthma, which can also affect academic performance.
The growing issue of childhood obesity can be slowed, if society focuses on the causes. There are many components that play into childhood obesity, some being more crucial than others. A combined diet and physical activity intervention conducted in the community with a school component is more effective at preventing obesity or overweight. Moreover, if parents enforce a healthier lifestyle at home, many obesity problems could be avoided. What children learn at home about eating healthy, exercising and making the right nutritional choices will eventually spill over into other aspects of their life. This will have the biggest influence on the choices kids make when selecting foods to consume at school and fast-food restaurants and choosing to be active. Focusing on these causes may, over time, decrease childhood obesity and lead to a healthier society as a whole.
Source of Support: Nil.
Conflict of Interest: None declared.
IMAGES
VIDEO
COMMENTS
There is mounting evidence that childhood obesity is a risk factor for the development of asthma. 42 A research study was conducted by Belamarich et al to investigate 1322 children aged 4 to 9 years with asthma. Obesity, as defined by the CDC, is the BMI, with weight and height being greater than the 95th percentile.
Society in general and primary care providers in particular are often highly biased toward people with obesity. 24 A study with obese children aged 9 to 11 years found implicit bias to be around 5%. 25 ... Future childhood obesity research should evaluate the best methods for educating primary care providers in providing family-centered care ...
Introduction. Childhood obesity is a major public health challenge, with one in three US children between the ages of 2 and 5 meeting criteria for overweight or obesity. 1 The urgency to reverse the course of childhood obesity has led to significant growth in the scientific literature evaluating childhood obesity interventions. Extant reviews of this research have provided limited guidance ...
The childhood obesity research that NIH supports includes studies in pregnancy, infancy, childhood, adolescence, and prevention and treatment approaches in families, schools, and other community settings, as well as in health care settings. The NIH also supports basic behavioral and social science research that is providing insights into ...
Despite the relative lack of widespread research in comparison to the adult population, newer therapies are being trialled, which should allow a greater availability of treatment options for childhood obesity in the future. This review summarizes the current evidence for the management of obesity in terms of medical and surgical options.
10.1542/6305605703112Video AbstractPEDS-VA_2021-0537086305605703112OBJECTIVES. Examine childhood obesity incidence across recent cohorts.METHODS. We examined obesity incidence and prevalence across 2 cohorts of children in the United States 12 years apart using the Early Childhood Longitudinal Studies, parallel data sets following the kindergarten cohorts of 1998 and 2010 with direct ...
Launched in 2009, the National Collaborative on Childhood Obesity Research (NCCOR) brings together four of the nation's leading research funders — the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH), the Robert Wood Johnson Foundation (RWJF), and the U.S. Department of Agriculture (USDA) — to accelerate progress in reducing childhood obesity in ...
This updated synthesis of obesity prevention interventions for children aged 6-18 years, found a small beneficial impact on child BMI for school-based obesity prevention interventions. A more comprehensive assessment of interventions is required to identify mechanisms of effective interventions to inform future obesity prevention public health policy, which may be particularly salient in for ...
Some studies comparing higher and lower infant formula protein content have reported that the higher protein group have a greater risk of subsequent obesity, especially in early childhood 41,42 ...
Childhood obesity rates have increased substantially over the past year in the UK, according to a new report from the UK Government's National Child Measurement Programme. This rise in prevalence is the largest single-year increase since the programme began 15 years ago and highlights the worldwide rising trend for obesity among children and adolescents. Once considered a problem mainly in ...
The annual incidence of obesity decreased from 5.4% during kindergarten to 1.7% between fifth and eighth grade. Overweight 5-year-olds were four times as likely as normal-weight children to become ...
In this phase 3a trial, which consisted of a 56-week treatment period and a 26-week follow-up period, we randomly assigned children (6 to <12 years of age) with obesity, in a 2:1 ratio, to receive ...
Introduction. Obesity in children and adolescents is a global health issue with increasing prevalence in low-income and middle-income countries (LMICs) as well as a high prevalence in many high-income countries. 1 Obesity during childhood is likely to continue into adulthood and is associated with cardiometabolic and psychosocial comorbidity as well as premature mortality.2, 3, 4 The provision ...
The Childhood Obesity Research Summit provided an overview of childhood obesity, and participants identified key questions that need to be answered, as well as recommendations for future work in the areas of education, public policy, and research. The recommendations and outcomes of the conference will help inform the American Heart Association ...
Childhood obesity. Approximately one third of the children and adolescents in the United States are either overweight or obese. Childhood obesity disproportionately affects specific racial and ethnic groups and households with low socioeconomic status and low parental education. The Alternative Learning Center (ALC) within Rochester School ...
Early childhood overweight and obesity is a major health concern affecting nearly a quarter of children in the United States, with similar rates in Europe, Canada and Australia (Morris et al., 2015), with Shakleton et al. (2018) reporting that New Zealand has among the highest rates in the world.Rudolf et al. (2019) has reported that as many as 10% of children in the United Kingdom are obese ...
Common challenges emerged across the workshops addressing measurement needs for childhood obesity. 10 These challenges (Figure 1) included improving processes for engaging multiple stakeholders and sectors to identify key measurement considerations; combining measurement of multiple factors within the same research or data system and across several levels to enhance understanding of complex ...
Equitable access to affordable, effective, and safe obesity prevention and treatment remains a problem for many children and families in the U.S. In 2023, the American Academy of Pediatrics (AAP) published its first Clinical Practice Guideline (CPG) for pediatric obesity evaluation and treatment, aiding the field's awareness of effective approaches. CDC has supported the adapting and ...
The childhood obesity research that NIH supports includes studies in pregnancy, infancy, childhood, adolescence, and prevention and treatment approaches in families, schools, and other community settings, as well as in health care settings. The NIH also supports basic behavioral and social science research that is providing insights into ...
For those whose mothers blood sugar was the least well controlled, the slowly improving to suboptimal group, the risk of childhood obesity was 30% higher. The study's authors conclude that swiftly ...
Joint action of ascorbic and humic acids in radical-chain oxidation of model hydrocarbons was studied. This effect is promising for development of complex directed-action preparations with controllable redox properties and development of antioxidants and pro-oxidants for medicinal purposes and technical applications.
Research studies have shown that obese individuals have a genetic variation that can influence their actions, such as increased food intake, ... which causes significant overlap between MS and features of normal growth. However, childhood obesity is associated with an inflammatory state even before puberty .
The research paper is aimed to modify the human health impact assessment of Cr in soils. The current article presents the input of ... A signicant number of studies have been devoted to the role of soil as one of the factors contributing to disease occur - rence (Alloway 2013; Li et al. 2019; Sevbitov et al. 2020;
Raise your hand if you've ever fallen off the monkey bars and hurt more than your pride. It's practically a childhood rite of passage. You climb, you swing, you push the limit, you miss, you cry ...
The first iteration of the Childhood Obesity Research Demonstration Projects (CORD 1.0), a program of research administered by the CDC, examined multi-sector intervention implementation in schools, community centers, early care and health centers, and pediatric primary care practices. ... from the Study of Latino Youth and the Hispanic ...
The study was aimed to estimate the relationship between the prevalence of allergic disease and helminth invasion by the trematode Opisthorchis felineus in rural and urban populations of Tomsk ...
Academia.edu is a platform for academics to share research papers. A pilot screening of prevalence of atopic states and opisthorchosis and their relationship in people of Tomsk Oblast ...
Childhood obesity has also been found to negatively affect school performance. A research study concluded that overweight and obese children were four times more likely to report having problems at school than their normal weight peers. They are also more likely to miss school more frequently, especially those with chronic health conditions ...